



Indications for Chest ultrasound include:
1.To differentiate white out of pleural effusion from consolidation
2. Bedside detection of anomalies to avoid transporting critically Ill patient and faster ,dynamic picture
3.Guidance for diagnostic and therapeutic thoracentesis.
A 3.5 to 5.0 MHz transducer.
Cardiac transducers are particularly effective allowing scanning between rib interspaces.
Typical Position in Critically Ill patient:- Supine with the ipsilateral arm held across the chest towards the opposite side.
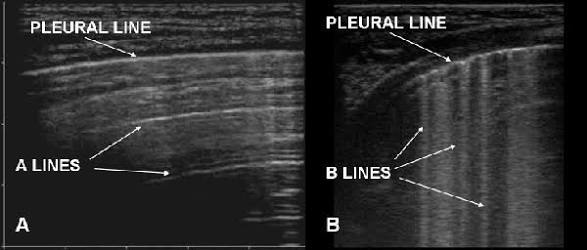
Method :-The transducer is oriented to scan between the ribs. The A lines and B lines are shown below:-
A lines:- A lines are horizontal lines that are brightly echogenic and located between the rib shadows when the probe is positioned longitudinally
B lines:- Pleural ultrasound image depicting B lines (“comet tail artifact”), which are seen in acute pulmonary edema and acute respiratory distress syndrome. The presence of B lines would provide an alternate explanation for increased density seen on the chest radiograph, other than pleural fluid.
Lung sliding — The sonographic effect of lung sliding (also known as lung gliding or the lung sliding sign) is created by movement of the lung relative to the chest wall during respiration . The sonographic appearance is that of a thin, bright line moving horizontally along the pleural line with a wave-like pattern located above (towards the chest wall) and a granular pattern below. Lung sliding is an indirect sign indicating adherence of the visceral pleura to the parietal pleura. When air separates the two pleural layers as in a pneumothorax, the movement disappears.
In addition the Blue Protocol can be downloaded from this link https://com-anest.sites.medinfo.ufl.edu/files/2015/06/2015-BLUELung.pdf which can be summarized as below:-
- Predominant A lines + lung sliding = Asthma/COPD
- Multiple predominant B lines anteriorly with lung sliding = Pulmonary Edema
- Normal anterior profile + DVT= PE
- Anterior absent lung sliding + A lines + lung point = Pneumothorax (PTX)
- Anterior alveolar consolidations, anterior diffuse B lines with abolished lung sliding, anterior asymmetric interstitial patterns, posterior consolidations or effusions with out anterior diffuse B lines = Pneumonia
- A lines:
- Appear as horizontal lines
- Indicate dry interlobular septa.
- Predominance of A lines has 90% sensitivity, 67% specificity for pulmonary artery wedge pressure <= 13mm Hg
- A line predominance suggests that intravenous fluids may be safely given without concern for pulmonary edema
- B lines (“comets”):
- White lines from the pleura to the bottom of the screen
- Highly sensitive for pulmonary edema, but can be present at low wedge pressures
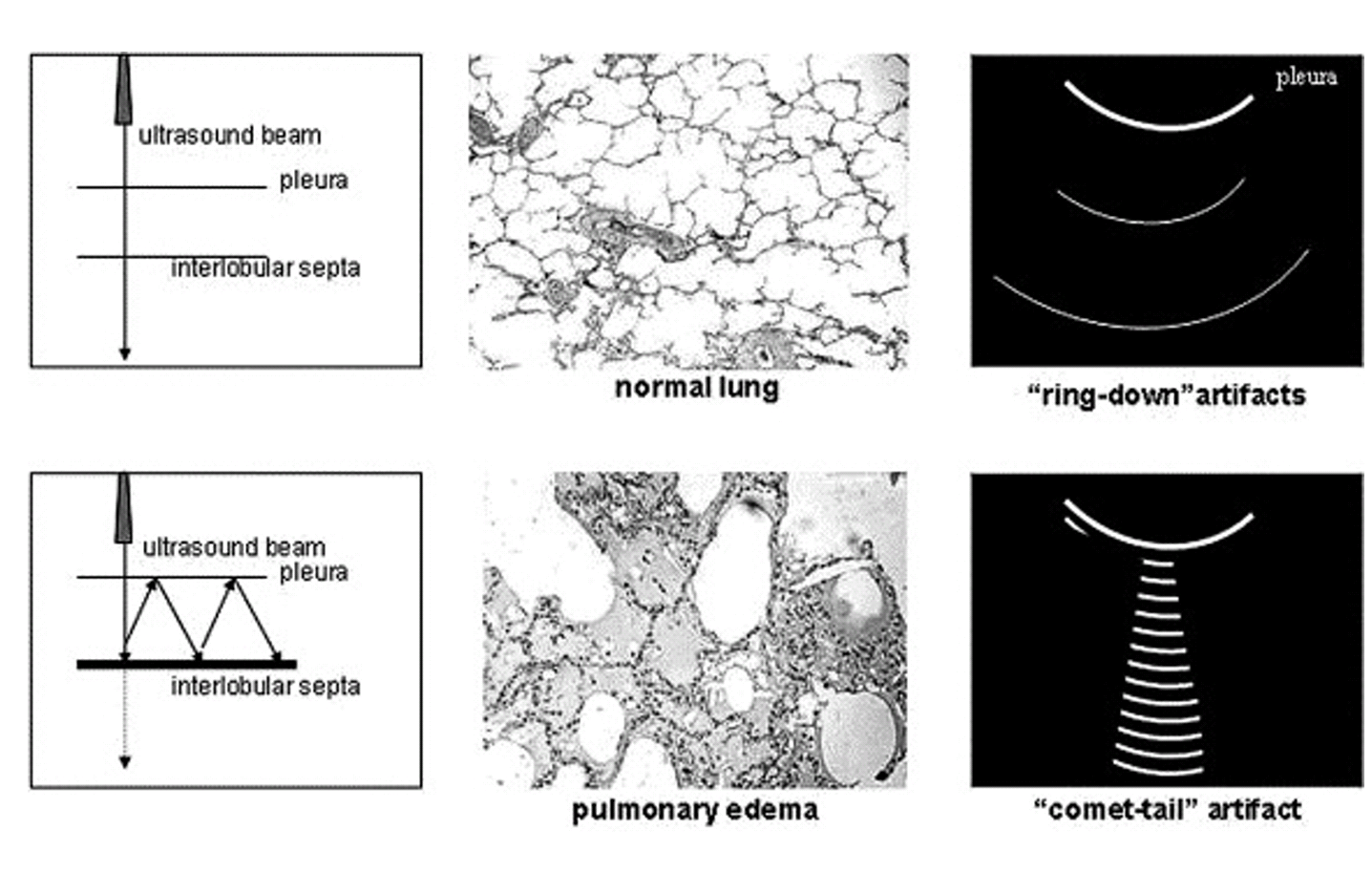
 The hypothesized physical and anatomic basis of echocardiographic lung comet tails. Reflections of the ultrasound beam between thickened interlobular septa and the pleura generate a resonance signal over a prolonged time. The increased return over time is interpreted by the ultrasound machine as a hyperechoic structure originating deeper in the tissue and is displayed as a comet-tail on the ultrasound screen. (Illustrations and images from Jambrik et al. Usefulness of ultrasound lung comets as a nonradiologic sign of extravascular lung water.
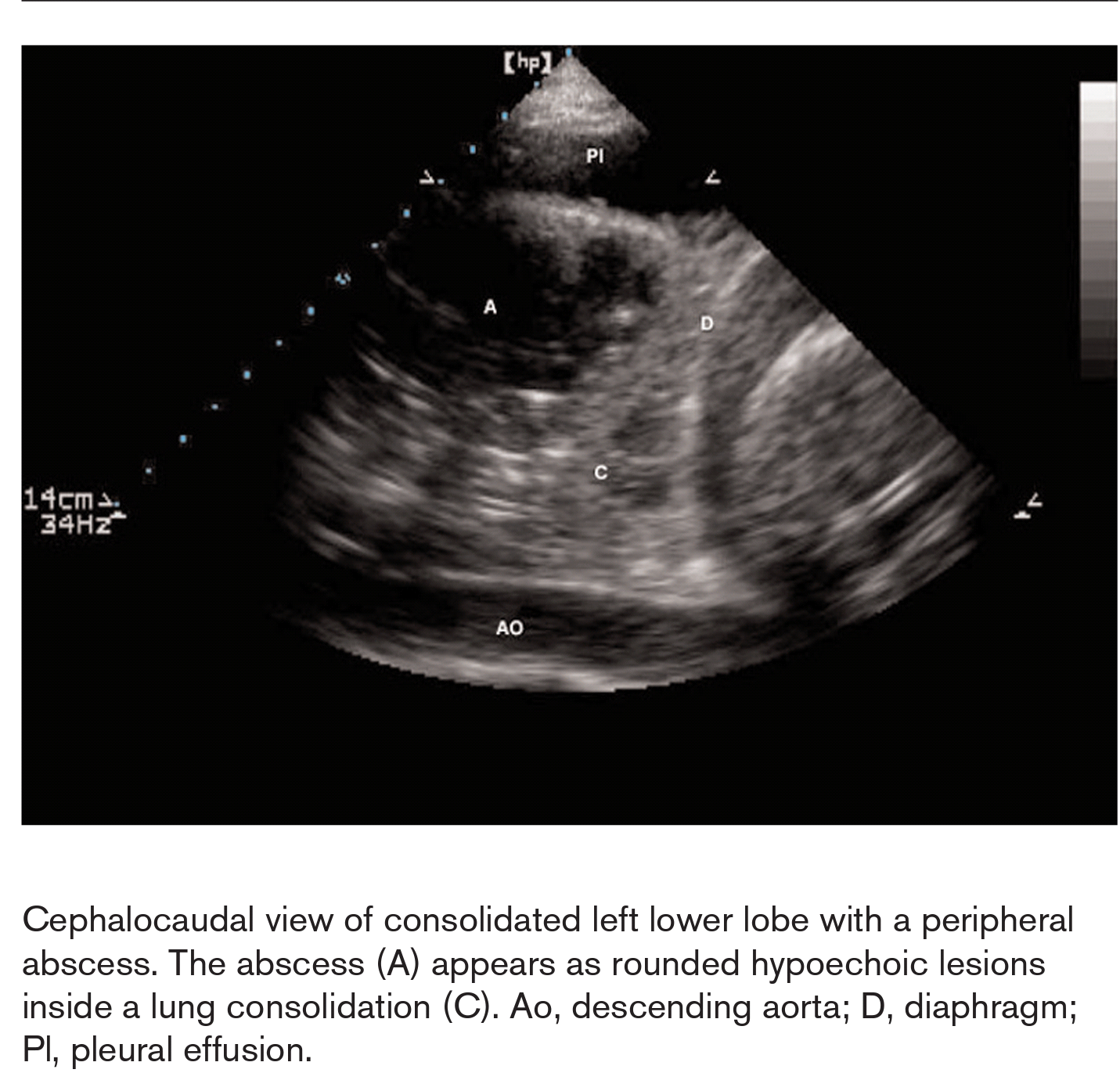
The hypothesized physical and anatomic basis of echocardiographic lung comet tails. Reflections of the ultrasound beam between thickened interlobular septa and the pleura generate a resonance signal over a prolonged time. The increased return over time is interpreted by the ultrasound machine as a hyperechoic structure originating deeper in the tissue and is displayed as a comet-tail on the ultrasound screen. (Illustrations and images from Jambrik et al. Usefulness of ultrasound lung comets as a nonradiologic sign of extravascular lung water. - Lung Abscess

This video shows a small pleural effusion and adjacent alveolar consolidation of the lung. With each inspiration, aerated lung is interposed into the imaging window with loss of visualization of the underlying structures. This is termed the curtain sign. The 3.5 MHz transducer is in longitudinal orientation and placed perpendicular to the chest wall to scan through the 8th intercostal space in the left mid-axillary line.
