



![]()
Posted by Dr KAMAL DEEP on June 7, 2026
Posted in Medical | Leave a Comment »
Posted by Dr KAMAL DEEP on May 27, 2026
Dear Colleagues,
I am writing this with a genuine sense of urgency and hope.
The NAMIC Study is not just another survey. It is an attempt to document the real ICU workforce and practice realities of India — across government hospitals, peripheral centres, district ICUs, teaching institutes, mixed-resource units, and regions that are usually never represented in national data.
If these voices are not captured now, they may once again remain invisible in future discussions, policies, and academic understanding of critical care in India.
At this stage, what matters most is not large numbers from the same institutions. Even a single response from a distant district, a government hospital, a peripheral ICU, or an underrepresented state can significantly strengthen the scientific and national value of this effort.
As colleagues many of you have professional and academic connections across the country. A simple forward from your side to the right person in the right region may help bring an entire unseen ICU ecosystem into this national dataset.
I sincerely request you not only to participate, but to help this study reach places that are otherwise rarely heard from.
Sometimes a single response can represent an entire region.
Survey Link:
https://forms.gle/1aFrVzbdbYhVmLJQ9
The study details and protocol are clearly mentioned within the form itself. The study has Institutional Ethics Committee (IEC) approval.
~NAMIC Study Team
Warm regards,
Posted in Medical | Leave a Comment »
Posted by Dr KAMAL DEEP on January 11, 2026
An 80-year-old woman with a long history of hypertension presented with progressive shortness of breath, markedly reduced urine output, and bilateral pedal edema over several days. She had been on chronic antihypertensive therapy with amlodipine and losartan and was taking aceclofenac daily for many years for chronic musculoskeletal pain. There was no history of recent hypotension or overt shock.
On examination, she was conscious, oriented, and hemodynamically stable, but tachypneic with bilateral basal crepitations and significant peripheral edema. Urine output was severely reduced. Laboratory investigations revealed serum creatinine 5.6 mg/dL, total leukocyte count 15.6 ×10⁹/L, and a markedly elevated procalcitonin of 50 ng/mL, suggestive of severe sepsis.
Ultrasound abdomen showed features of chronic kidney disease with chronic liver disease and ascites. CT chest demonstrated cardiomegaly with pulmonary congestion, consistent with fluid overload.
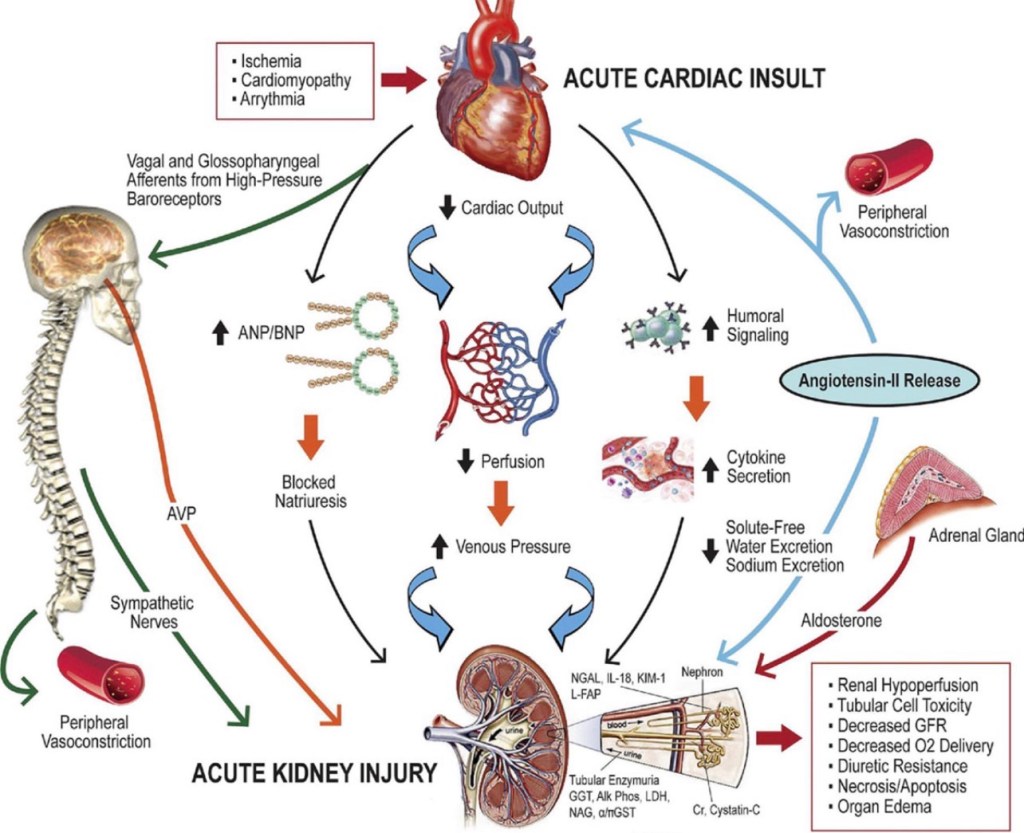
The presentation was interpreted as acute oligo-anuric AKI on CKD, occurring in the setting of acute cardiorenal syndrome. Long-standing hypertensive heart disease had resulted in diastolic dysfunction (HFpEF), leading to pulmonary congestion and renal venous congestion, thereby reducing effective renal perfusion. Superimposed chronic NSAID use caused prostaglandin inhibition with afferent arteriolar constriction, while chronic losartan therapy resulted in efferent arteriolar dilation. The combined effect of reduced inflow, increased outflow, and elevated venous back-pressure led to collapse of glomerular filtration pressure, explaining the patient’s oligo-anuria and poor diuretic responsiveness.
The associated chronic liver disease was attributed to long-standing hepatic venous congestion (congestive hepatopathy) secondary to chronic cardiac dysfunction, likely accelerated by recurrent subclinical hypoperfusion and long-term NSAID exposure, completing a cardio-hepato-renal syndrome. Given severe oligo-anuria, fluid overload with respiratory compromise, and sepsis-associated ATN, the patient was planned for early renal replacement therapy as physiologic support rather than rescue therapy.
Teaching point:
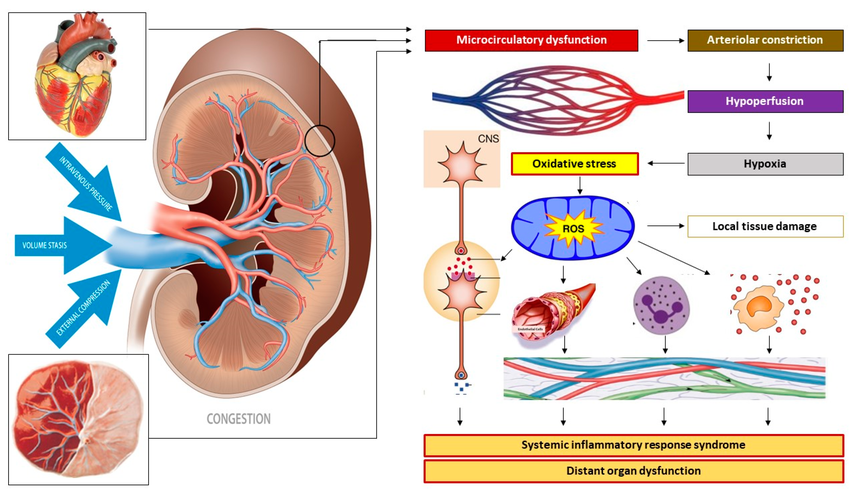
Mechanisms of venous congestion at the level of the kidney. Venous congestion can result from venous vascular hypertonia with subsequent venous hypertension, from volume stasis arising from (sub-)obstructed outflow, and/or from external compression. At the level of the kidneys, this congestion induces a retrograde dysfunction of the peritubular and glomerular capillaries. Reflex arteriolar constriction and activation of the renin–angiotensin–aldosterone system prevents further microcirculatory deterioration at the cost of reduced organ perfusion and subsequent parenchymal hypoxia. An oxidative stress response induces immunological, neurological, and metabolic protection mechanisms by activating the autonomic nervous system and the intravascular distribution of cytokines, endocrines, and vasoactive mediators, causing endothelial activation and a generalized state of inflammation. In non-pregnant individuals, this sequence of events unfolds in the kidneys as part of the pathophysiology of renocardial syndrome but can also occur in other internal organs as in cardiohepatic or hepatorenal syndromes. In pregnancy, this mechanism may unfold in the uterus and placenta as well as in internal organs. In this picture, the kidney may serve as a proxy for other maternal organs, such as uterus-placenta, heart, etc.
Posted in Medical | Leave a Comment »
Posted by Dr KAMAL DEEP on July 22, 2025
From Saline to Balanced: My Shift as an Intensivist, and What DKA Taught Me About Acid-Base
A few years ago, I was what you’d call a “saline intensivist.” Like many of us trained in the fast-paced world of critical care, I reached for normal saline as my default resuscitation fluid. It was reliable, familiar, and widely available. But over time—and with a growing body of evidence—I’ve come to understand that “normal” saline isn’t always physiological, especially when it comes to complex acid-base disorders like diabetic ketoacidosis (DKA).
Today, I practice more as a “balanced intensivist,” and DKA is one of the classic cases that illustrates why fluid choice matters.
DKA: The Classic High-Anion Gap Acidosis
In DKA, the absence of insulin drives the body to burn fat for energy, leading to the accumulation of ketone bodies like beta-hydroxybutyrate and acetoacetate. These organic acids overwhelm the buffering capacity of the body, consuming bicarbonate and resulting in a high-anion gap metabolic acidosis (HAGMA).
At this stage, the acidosis is caused by too many acids, not the loss of base.
The Shift: From HAGMA to NAGMA During Recovery
As we begin treatment—with insulin and fluids—the production of ketones stops. The kidneys then begin to excrete the excess ketone anions in the urine. But here’s the catch: those ketones are actually bicarbonate precursors. If retained, they would eventually regenerate bicarbonate as they are metabolized.
When they’re lost in the urine—along with sodium or potassium—we also lose the potential to regenerate bicarbonate. This is functionally equivalent to losing base, not adding acid.To maintain electrical balance, the kidneys start retaining chloride.
And if we’re giving large volumes of 0.9% normal saline, which already contains 154 mmol/L of chloride, we’re further loading the system with chloride.
The result? A normal anion gap metabolic acidosis (NAGMA)—also called hyperchloremic acidosis. The original ketone-driven HAGMA has resolved, but the patient now has a new, iatrogenic acidosis driven by bicarbonate loss and chloride gain.
Balanced Crystalloids: More Than Just a Trend
Balanced salt solutions like Ringer’s lactate have a lower chloride content and include buffering agents like acetate or lactate that are metabolized to bicarbonate. They’re less likely to cause or worsen hyperchloremic acidosis, especially in the DKA recovery phase.
Several studies—including SPLIT, SALT-ED, and SMART—have consistently shown benefits of balanced fluids in terms of acid-base balance, kidney outcomes, and even mortality in some subgroups. While not DKA-specific, the logic applies cleanly here.
So Why Did I Switch?
Because I saw it with my own eyes.
I saw patients recover from DKA only to remain acidotic from fluids we gave them. I saw chloride levels climb while bicarbonate remained stubbornly low. And I saw that simply switching from saline to a balanced solution often helped correct that persistent acidosis faster—and more physiologically.
Key Takeaways for Clinicians
In early DKA, acidosis is due to ketone accumulation (HAGMA). During recovery, renal loss of ketone salts (which are bicarbonate precursors) leads to bicarbonate depletion. Chloride retention, especially from normal saline, replaces the lost bicarbonate, causing a normal anion gap metabolic acidosis (NAGMA). Balanced fluids reduce this risk by supplying less chloride and offering bicarbonate precursors.
Final Thoughts
We often think of fluids as neutral tools, but in critical care, fluids are drugs. Their composition, volume, and timing all matter. In DKA, understanding the physiology of acid-base balance during recovery can help us choose fluids more wisely—and avoid replacing one problem with another.
I used to be a saline intensivist.
Now, I’m balanced.
Posted in Medical | Tagged: balanced salt solution, NAGMA in DKA | Leave a Comment »
Posted by Dr KAMAL DEEP on March 9, 2025
Introduction: The Complex Role of Protein in ICU Patients
For decades, ICU nutrition guidelines emphasized high protein intake (≥1.5 g/kg/day) to combat muscle wasting, malnutrition, and immune dysfunction in critically ill patients. However, recent landmark RCTs and meta-analyses have challenged the belief that “more protein is always better.”
Definition of Sarcopenia
• Consensus Definitions:
Major working groups such as the European Working Group on Sarcopenia in Older People (EWGSOP) and the Asian Working Group for Sarcopenia (AWGS) define sarcopenia as a condition involving both low muscle quantity and low muscle function (either strength or performance).
• Probable Sarcopenia: Identified by low muscle strength (commonly measured by handgrip strength).
• Confirmed Sarcopenia: When low muscle mass is also present.
• Severe Sarcopenia: When there is low muscle mass, low muscle strength, and poor physical performance (e.g., slow gait speed).
Methods to Measure Sarcopenia
1. Imaging Techniques for Muscle Mass
• Dual-Energy X-ray Absorptiometry (DXA):
• Pros: Widely used; provides detailed body composition analysis.
• Cons: Requires patient transfer and specialized equipment; less practical in critically ill patients.
• Computed Tomography (CT) and Magnetic Resonance Imaging (MRI):
• Pros: Considered gold standards for measuring muscle cross-sectional area; excellent image quality.
• Cons: Exposure to radiation (CT), high cost, and impractical for repeated bedside evaluations.
• Ultrasound:
• Pros: Non-invasive, portable, and repeatable at the bedside.
• How It’s Done:
• Site: The rectus femoris muscle of the thigh is commonly used.
• Technique:
• Patient Positioning: Patient is in a supine position with the knee extended and relaxed.
• Landmarks: Measure at the midpoint between the anterior superior iliac spine (ASIS) and the patella.
• Probe: A high-frequency linear probe (7–12 MHz) is used.
• Measurements:
• Muscle Thickness (RF-MLT): Distance between the superficial and deep fascia layers of the muscle.
• Cross-Sectional Area (RF-CSA): Outline the muscle boundary to calculate area.
• Interpretation: A reduction of more than 10% in muscle thickness over 7 days is often considered indicative of significant muscle wasting, which correlates with sarcopenia and poorer outcomes.
• Bioelectrical Impedance Analysis (BIA):
• Pros: Quick and easy; provides estimates of fat-free mass.
• Cons: Accuracy can be affected by fluid shifts common in critically ill patients.
2. Functional Measures
• Handgrip Strength:
• Method: Use a dynamometer to measure the maximum voluntary contraction of the hand.
• Thresholds (EWGSOP2): Common cutoffs are <27 kg for men and <16 kg for women in older adults, though ICU-specific thresholds might differ.
• Significance: Reduced grip strength is a strong predictor of sarcopenia and overall functional decline.
• Physical Performance Tests:
• Tests such as gait speed or the Short Physical Performance Battery (SPPB) are used in ambulatory patients but are often not feasible in critically ill, immobilized patients.
Because sarcopenia encompasses both muscle mass and muscle function, the diagnosis is typically made by combining measurements:
• Step 1: Screening for low muscle strength (e.g., low handgrip strength).
• Step 2: Confirming low muscle mass through imaging (ultrasound, DXA, CT) or body composition analysis (BIA).
• Step 3: Assessing physical performance (if possible), to gauge the severity.
Integration with Nutritional Assessments:
Tools like GLIM, NRS-2002, and mNUTRIC incorporate various parameters (e.g., weight loss, BMI, decreased food intake, severity of illness) to assess nutritional risk. Although these tools have limitations in the ICU (due to fluid shifts and rapid metabolic changes), they can be complemented by direct muscle measurements to provide a fuller picture of a patient’s nutritional and functional status.
• Implications for Treatment:
Early identification of sarcopenia through ultrasound and functional tests can lead to timely interventions, such as adjusting protein intake, initiating early mobilization, and using anabolic agents or nutritional supplements (e.g., HMB) to preserve muscle mass.
This article will cover:
✅ What does the latest research say about protein intake in ICU patients?
✅ How does malnutrition impact ICU outcomes, and how can we assess it?
✅ Why might excessive protein be harmful in conditions like AKI?
✅ What are the molecular mechanisms of muscle wasting in ICU patients?
✅ How can bedside ultrasound help monitor muscle loss?
✅ What is the optimal protein dosing strategy for different ICU populations?
By the end, we’ll establish a personalized, evidence-based approach to ICU protein nutrition.
1. The Burden of Malnutrition in ICU Patients
Malnutrition is common in ICU patients due to:
🔹 Hypermetabolism & catabolic stress (sepsis, trauma, burns)
🔹 Reduced oral/enteral intake (NPO status, GI dysfunction)
🔹 Muscle breakdown from immobilization & inflammation
📊 Key Facts:
• Up to 60% of ICU patients develop malnutrition within 48 hours of admission
• Malnourished ICU patients have:
🚨 Higher mortality (30–50%)
🚨 Longer mechanical ventilation & ICU stay
🚨 Greater risk of ICU-acquired weakness (ICUAW)
How Do We Assess Malnutrition in ICU Patients?
🔹 1. GLIM Criteria (Global Leadership Initiative on Malnutrition)
📌 Two-Step Diagnosis:
1️⃣ Phenotypic Criteria (Need at least 1)
• Weight loss (>5% in 6 months or >10% in 1 year)
• Low BMI (<20 if <70 years, <22 if >70 years)
• Reduced muscle mass (via ultrasound, CT, bioimpedance)
2️⃣ Etiologic Criteria (Need at least 1)
• Reduced food intake/absorption (>50% of needs for >1 week)
• Systemic inflammation (sepsis, burns, major surgery)
🚀 Patients meeting 1 phenotypic + 1 etiologic criterion = Malnutrition diagnosis
🔹 2. NRS-2002 (Nutritional Risk Screening – 2002)
📌 Used in ICU to screen for malnutrition risk
🔹 Scoring System (0–6 points):
✔ Nutritional Status (0-3 points) → Weight loss, BMI, intake reduction
✔ Disease Severity (0-3 points) → Sepsis, major surgery, ICU stay
✔ Age ≥70 years → Add +1 point
📌 Scores ≥3 indicate malnutrition risk → Early nutrition therapy needed
🔹 3. mNUTRIC Score (Modified Nutrition Risk in Critically Ill)
📌 Designed for ICU patients to predict mortality risk
🔹 Includes:
✔ APACHE II / SOFA score
✔ Age, BMI, number of comorbidities
✔ Days from ICU admission to nutrition initiation
🚀 mNUTRIC ≥5 = High risk → Early aggressive nutrition needed
2. ICU-Acquired Weakness (ICUAW): Causes & Prevention
What Causes ICUAW?
🚨 Critical illness leads to a combination of:
• Inflammation-induced muscle breakdown (TNF-α, IL-6, IL-1β)
• Corticosteroid-induced myopathy
• Mitochondrial dysfunction
• Insulin resistance & anabolic resistance
• Disuse atrophy from bed rest
📊 Up to 50% of ventilated ICU patients develop ICUAW, leading to:
🚨 Delayed ventilator weaning
🚨 Longer ICU stay
🚨 Increased 1-year mortality
3. Molecular Mechanisms of Muscle Loss in ICU Patients
✅ Muscle protein synthesis is impaired due to:
• mTOR inhibition by inflammatory cytokines
• Suppression of IGF-1 (growth factor needed for muscle regeneration)
🚨 Muscle breakdown is accelerated due to:
• Activation of Ubiquitin-Proteasome System (UPS)
• Mitochondrial dysfunction leading to oxidative stress
🔬 Anabolic resistance → Even with high protein intake, ICU patients fail to utilize amino acids efficiently.
4. What Do Major Clinical Trials Say About ICU Protein Needs?
Major Clinical Trials: The High-Protein Controversy
🔹 EFFORT Trial (2023, The Lancet)
“More Protein Didn’t Improve Outcomes—And May Have Harmed Some Patients.”
• Study Design: Large multicenter RCT (85 ICUs, 1,301 patients)
• Intervention: High protein (2.2 g/kg/day) vs. Standard protein (1.2 g/kg/day)
• Primary Outcome: No difference in time-to-discharge-alive (p=0.27)
🔍 Key Findings:
🚨 High protein worsened outcomes in AKI patients (HR 1.12, 95% CI: 1.02–1.27)
🚨 No benefit in mortality, ventilator-free days, or infections
📌 Takeaway: Very high protein (>2.2 g/kg/day) might be harmful, especially in AKI & multi-organ failure patients.
🔹 TARGET Trial (2018, NEJM)
“More Calories Did Not Improve Survival.”
• Study Design: Multicenter RCT (3,957 ICU patients)
• Intervention: High-energy EN (1.5 kcal/ml) vs. Standard EN (1 kcal/ml)
• Primary Outcome: No difference in 90-day mortality
🔍 Key Findings:
❌ Higher calorie intake did not reduce ICU mortality or ventilator duration
❌ No reduction in infections or complications
📌 Takeaway: Caloric overfeeding is ineffective—protein needs should be separately optimized.
🔹 NUTRIREA-2 Trial (2018, JAMA)
“Route of Feeding Matters More Than the Protein Dose.”
• Study Design: Multicenter RCT (2,400 ICU patients)
• Intervention: Early Enteral Nutrition (EN) vs. Early Parenteral Nutrition (PN)
• Primary Outcome: No difference in 28-day mortality
🔍 Key Findings:
🚨 EN group had more GI complications (vomiting, diarrhea, aspiration pneumonia)
🚨 PN group had more bloodstream infections
📌 Takeaway: EN remains the preferred route, but careful monitoring for GI intolerance is needed.
🔹 2024 Meta-Analysis (Lee et al.)
“High Protein Increased Mortality in AKI Patients.”
• Data: 23 RCTs, 3,303 ICU patients
• Primary Outcome: No mortality benefit of high protein overall
🔍 Key Findings:
🚨 Increased mortality in AKI patients (42% higher risk, NNH = 7)
✅ High protein preserved muscle mass but increased nitrogen waste
📌 Takeaway: Moderate protein (~1.2–1.5 g/kg/day) is safest, while AKI patients should receive ≤1.2 g/kg/day.
However, excessive protein intake may:
❌ Increase metabolic waste (urea, nitrogen load), worsening AKI
❌ Cause unintended hyperglycemia (via gluconeogenesis)
❌ Fail to translate into better survival outcomes (as seen in recent trials)
Study
Protein Intake
Key Findings
EFFORT (2023, Lancet)
2.2 g/kg/day vs. 1.2 g/kg/day
Higher protein increased mortality in AKI patients (p=0.005) 🚨 No benefit in ICU/hospital stay ❌
TARGET (2018, NEJM)
High-calorie EN (1.5 kcal/ml) vs. Standard EN (1 kcal/ml)
No survival benefit of increased calorie intake ❌
NUTRIREA-2 (2018, JAMA)
Early EN vs. Early PN
No difference in mortality, but EN caused more GI issues ❌
Meta-Analysis (2024, Lee et al.)
1.5 g/kg/day vs. 0.92 g/kg/day
🚨 High protein increased AKI mortality by 42% (NNH = 7) ❌ No mortality benefit overall
📌 Takeaway: Moderate protein (1.2–1.5 g/kg/day) is safest, while AKI patients should receive ≤1.2 g/kg/day.
5. Bedside Ultrasound for Muscle Monitoring in ICU
✅ Rectus Femoris ultrasound (RF-US) is the best tool for real-time muscle loss assessment.
📊 How to interpret:
📉 >10% muscle loss in 7 days → ICUAW risk
📉 >15% loss over ICU stay → Long-term disability risk
🔬 Combining nutrition + rehab (electrical stimulation, resistance exercise) improves muscle preservation.
6. Practical ICU Protein Guidelines Based on Current Evidence
Patient Type
Protein Intake
General ICU Patients
1.2–1.5 g/kg/day
Sepsis, Trauma, Burns
1.5–2.5 g/kg/day
AKI (No CRRT)
≤1.2 g/kg/day
CRRT (Dialysis Patients)
2.0–2.5 g/kg/day
The ESPEN guidelines on clinical nutrition in the ICU provide several key recommendations on protein intake, timing, and considerations for different patient groups. Here are the most relevant points extracted from the document:
Protein Intake Recommendations
• General ICU Patients: ESPEN recommends 1.3 g/kg protein equivalents per day during critical illness, delivered progressively .
• Sepsis & Septic Shock: ESPEN does not provide a single definitive target but suggests avoiding overfeeding, as septic patients may not benefit from increased protein intake (1.2 g/kg/d) compared to non-septic patients, though no harm was reported either .
• Acute Kidney Injury (AKI): Traditional recommendations suggest 1.2-1.5 g/kg/d, but some studies indicate that higher protein intake might be associated with worse outcomes in AKI patients not receiving renal replacement therapy .
• Sarcopenic ICU Patients: Those with muscle loss may benefit more from >1.2 g/kg/day protein intake .
• Parenteral Nutrition (PN): ESPEN suggests that PN should be used if enteral nutrition (EN) is insufficient after three days. Overfeeding should be avoided in the first days of ICU admission
1. Acute Phase of Sepsis:
During the initial acute phase (first 24–96 hours), it’s recommended to provide a protein intake of approximately 1.0 g/kg/day. This approach aims to balance the need for protein while avoiding potential adverse effects associated with higher protein delivery during this critical period.
2. Post-Acute Phase of Sepsis:
After the acute phase, as the patient stabilizes, increasing protein intake becomes crucial to minimize muscle loss and support recovery. Guidelines suggest aiming for a protein intake of 1.2–2.0 g/kg/day during this period.
3. Recovery Phase:
In the recovery phase, particularly for patients engaging in rehabilitation and physical therapy, protein requirements may further increase. Some recommendations advocate for protein intakes up to 2.0 g/kg/day to support muscle rebuilding and overall recovery.
Clinical Evidence Supporting Higher Protein Intake:
• A retrospective study observed that patients with sepsis who received higher protein intake during the first week had a lower in-hospital mortality rate. Specifically, an average daily protein intake was associated with a reduced risk of in-hospital death.
• The ESPEN guidelines on clinical nutrition in the ICU highlight that protein intakes greater than 1.2 g/kg/day are associated with improved outcomes in critically ill patients, including those with sepsis.
It’s important to note that while higher protein intake is beneficial during the post-acute and recovery phases, individual patient factors such as kidney function, metabolic status, and overall clinical condition should guide specific protein targets. Close monitoring and adjustment of nutritional strategies are essential to optimize outcomes in septic patients.
🚀 The future isn’t “more protein” but “right protein, right patient, right time.”
📌 Final Thought: ICU nutrition must be tailored—not just based on general guidelines, but on real-time patient responses.
Extras
Detailed Overview of HMB (β-Hydroxy β-Methylbutyrate) in ICU Patients
HMB (β-Hydroxy β-Methylbutyrate) is a metabolite of leucine that has been widely studied for its muscle-preserving and anabolic effects in critically ill patients. Below is a comprehensive review of its mechanism of action, clinical benefits, side effects, and landmark studies supporting its use.
1. Mechanism of Action: How HMB Works in ICU Patients
HMB exerts multiple beneficial effects in critically ill, immobilized, and muscle-wasting patients through the following mechanisms:
(A) Stimulation of Muscle Protein Synthesis (mTOR Activation)
✅ HMB activates the mTOR pathway, which is the key regulator of muscle growth.
✅ This leads to increased muscle protein synthesis (MPS) → Helps maintain lean body mass.
✅ Unlike leucine, HMB is more potent in stimulating MPS because it bypasses certain metabolic steps.
📌 Supporting Study:
• Eley et al. (2008): HMB increased muscle protein synthesis by 30% in septic rats.
(B) Inhibition of Muscle Protein Breakdown (Ubiquitin-Proteasome Pathway Suppression)
✅ Critical illness activates the Ubiquitin-Proteasome System (UPS) → leading to muscle proteolysis (breakdown).
✅ HMB directly inhibits UPS, preventing excessive protein degradation.
✅ This helps preserve muscle mass even during immobilization or sepsis.
📌 Supporting Study:
• Smith et al. (2005): HMB reduced muscle protein breakdown by 50% in cachectic cancer patients.
(C) Anti-Inflammatory Effects (↓ TNF-α, IL-6, IL-1β)
✅ Critical illness triggers systemic inflammation (sepsis, trauma, burns), leading to muscle wasting.
✅ HMB reduces pro-inflammatory cytokines (IL-6, TNF-α, IL-1β) → Improves muscle retention.
✅ HMB also preserves mitochondrial function, reducing oxidative stress.
📌 Supporting Study:
• Hsieh et al. (2006): ICU patients receiving HMB-enriched nutrition had a 59% reduction in CRP (inflammatory marker).
(D) Enhancing Immune Function & Wound Healing
✅ HMB supports immune cell function by maintaining glutathione levels.
✅ Stimulates collagen synthesis → Improves wound healing in post-surgical ICU patients.
📌 Supporting Study:
• Clark et al. (2000): HMB improved wound healing & reduced hospital stay in elderly ICU patients.
2. Clinical Benefits of HMB in ICU Patients
HMB is particularly useful in catabolic ICU conditions where muscle loss is rapid and severe.
✅ Preserves Muscle Mass & Strength
• ICU patients lose 2-4% of muscle mass per day due to immobilization.
• HMB supplementation slows down this muscle loss by inhibiting protein breakdown.
• Deutz et al. (2013): HMB prevented significant muscle atrophy in ICU patients receiving high-protein enteral nutrition.
✅ Reduces ICU-Acquired Weakness (ICU-AW)
• ICU-AW affects 40-50% of critically ill patients, leading to long-term disability.
• HMB supplementation improves functional outcomes (grip strength, mobility).
• NOURISH Trial (2016): ICU patients receiving HMB-enriched oral nutrition supplements (ONS) had a 50% lower 90-day mortality.
✅ Supports Recovery Post-ICU (Rehabilitation Phase)
• Post-ICU patients continue losing muscle for weeks to months after discharge.
• HMB combined with physiotherapy accelerates muscle recovery & reduces re-hospitalization.
• Deutz et al. (2021): ICU patients receiving HMB showed improved physical function at 30 days post-discharge.
3. Landmark Studies Supporting HMB Use in ICU
Study
Key Findings
Clinical Impact
Deutz et al. (2013)
HMB preserved muscle mass in ICU patients receiving high-protein EN.
Supports HMB in ICU nutrition.
NOURISH Trial (2016)
HMB-enriched ONS reduced 90-day mortality by 50%.
Strong evidence for HMB in ICU recovery.
Hsieh et al. (2006)
CRP reduced by 59% in ICU patients receiving HMB.
HMB has anti-inflammatory benefits.
Eley et al. (2008)
HMB increased muscle protein synthesis by 30% in sepsis.
Supports HMB in ICU-acquired weakness.
Clark et al. (2000)
HMB improved wound healing & recovery in ICU.
Useful in post-surgical patients.
📌 Takeaway:
HMB has well-documented benefits for ICU patients, including muscle preservation, inflammation reduction, and improved recovery.
4. HMB Dosage & Administration in ICU
Route
Recommended Dose
Duration
Oral / Enteral (EN)
3 g/day (divided into 2-3 doses)
Minimum 7-14 days, ideally 4-6 weeks
Parenteral (IV HMB not widely available)
Not routinely used
–
📌 Best Administered With:
✔ High-protein EN (whey/casein) → Enhances muscle anabolism.
✔ Omega-3s (EPA/DHA) → Synergistic anti-inflammatory effect.
5. Potential Side Effects of HMB
HMB is very safe, but some mild side effects have been reported:
Side Effect
Frequency
Clinical Relevance
Mild GI Discomfort (bloating, diarrhea)
Rare (<5% of patients)
Dose-dependent, resolves with lower dose
Hypoglycemia Risk (in diabetics)
Low
Monitor blood sugar in insulin-dependent patients
No Liver/Kidney Toxicity
None reported
Safe for long-term ICU use
📌 Safety Summary:
✔ HMB has no major side effects.
✔ Safe in elderly, renal failure, and chronic ICU patients.
✔ Can be continued post-ICU to aid rehabilitation.
6. Final Takeaways
✔ HMB is a potent muscle-preserving agent, working via mTOR activation & protein breakdown inhibition.
✔ HMB reduces inflammation, improving ICU recovery.
✔ HMB supplementation (3 g/day) is recommended in critically ill patients at risk of muscle loss.
✔ Safe, with no major side effects (unlike anabolic steroids).
✔ HMB should be combined with high-protein nutrition + physiotherapy for best results.
Vanhorebeek I, et al. (2020) – ICU-Acquired Weakness Review
🔹 Objective:
• Comprehensive review of ICU-acquired weakness (ICU-AW), its mechanisms, and interventions.
🔹 Key Findings:
• ICU-AW is caused by sepsis, hyperglycemia, neuromuscular blockers, and prolonged immobility.
• 40% of ICU patients develop ICU-AW; in surgical ICUs, this rate is 56-74%.
🔹 Clinical Impact:
• Early mobilization, nutrition (≥1.5 g/kg protein/day), and glucose control are key to preventing ICU-AW.
📌 Reference: Vanhorebeek I, et al. Intensive Care Med. 2020;46(4):637-53
Appleton RT, et al. (2015) – Incidence of ICU-AW
🔹 Objective:
• Systematic review analyzing the prevalence of ICU-AW in critically ill patients.
🔹 Key Findings:
• 4 out of 10 critically ill patients develop ICU-AW.
• ICU-AW significantly delays recovery and increases mortality.
🔹 Clinical Impact:
• ICU patients should undergo early screening for weakness & receive aggressive rehabilitation.
📌 Reference: Appleton RT, et al. J Intensive Care Soc. 2015;16(2):126-36
Wang W, et al. (2020) – ICU-AW & Nutrition
🔹 Objective:
• Reviewed nutritional strategies for ICU-AW patients.
🔹 Key Findings:
• Early enteral nutrition (EN) is superior to PN unless contraindicated.
• Delaying PN for 7 days reduces infection risk (EPaNIC Trial).
🔹 Clinical Impact:
• Reinforces ESPEN guidelines recommending early EN over PN in critically ill patients.
📌 Reference: Wang W, et al. Front Med (Lausanne). 2020;7:559789
Lees et al. (2024) – Muscle Loss in ICU Patients
🔹 Objective:
• Examined muscle wasting trends in critically ill patients across different conditions.
🔹 Key Findings:
• ICU patients lose ~2% of muscle mass per day in the first week.
• 15% muscle loss in 1 week → ICU-AW develops in ~50% of patients.
🔹 Clinical Impact:
• Supports high-protein feeding (1.5-2.0 g/kg/day) & resistance training in ICU.
📌 Reference: Lees et al. Crit Care Clin. 2024
Yuan G, et al. (2021) – ICU-AW & Muscle Mass
🔹 Objective:
• Investigated erector spinae muscle cross-sectional area in ICU-AW patients.
🔹 Key Findings:
• Significant muscle atrophy seen as early as day 7 of ICU stay.
• Worse prognosis in ICU patients with severe muscle loss.
🔹 Clinical Impact:
• ICU teams should monitor muscle loss using imaging & functional assessments.
📌 Reference: Yuan G, et al. Medicine (Baltimore). 2021;100(47):e27806
Prado CM, et al. (2023) – Muscle’s Role in Metabolism
🔹 Objective:
• Analyzed muscle’s role as a metabolic organ & its impact on ICU recovery.
🔹 Key Findings:
• Muscle regulates glycemic control, immune function, and inflammation.
• Severe muscle loss post-ICU increases mortality & disability.
🔹 Clinical Impact:
• ICU recovery strategies must include nutritional & resistance training approaches.
📌 Reference: Prado CM, et al. JPEN J Parenter Enteral Nutr. 2023
He Y, et al. (2019) – ONS & Surgical Site Infection in Orthopedic Patients
🔹 Objective:
• Evaluated whether ONS can reduce postoperative infections and readmission rates in elderly orthopedic patients with hypoalbuminemia.
🔹 Key Findings:
• ONS reduced 30-day readmission risk by 78%.
• Lower incidence of prosthetic joint infection.
🔹 Clinical Impact:
• ONS should be routinely provided postoperatively to improve nutritional status and lower infection risks.
📌 Reference: He Y, et al. J Orthop Surg Res. 2019;14(1):292
Deutz NE, et al. (2021) – ONS & Handgrip Strength
🔹 Objective:
• Studied the effect of ONS on muscle strength (handgrip) in ICU patients with chronic obstructive pulmonary disease (COPD).
🔹 Key Findings:
• ONS improved handgrip strength significantly at day 30 post-discharge.
• CRP (inflammatory marker) levels decreased by 59%, indicating reduced systemic inflammation.
🔹 Clinical Impact:
• Suggests ONS has both anabolic and anti-inflammatory benefits for critically ill patients.
📌 Reference: Deutz NE, et al. Clin Nutr. 2021;40(3):1388-95
Deutz NE, et al. (2016) – NOURISH Trial: ONS & ICU Recovery
🔹 Objective:
• Evaluated the impact of specialized oral nutritional supplements (ONS) on mortality and readmission rates in malnourished hospitalized older adults.
🔹 Key Findings:
• ONS significantly reduced 90-day mortality.
• Improved handgrip strength & body weight at day 30.
• Reduced hospital readmission rates.
🔹 Clinical Impact:
• Supports the use of high-protein ONS in ICU recovery to reduce mortality and improve muscle strength.
📌 Reference: Deutz NE, et al. Clin Nutr. 2016;35(1):18-26
Posted in Medical | Leave a Comment »
Posted by Dr KAMAL DEEP on February 26, 2025
Percutaneous dilatational tracheostomy (PDT) has revolutionized airway management in intensive care units (ICUs). Its minimally invasive nature, ability to be performed bedside, and cost-effectiveness make it a preferred choice for patients requiring prolonged ventilation. However, as simple as it may seem, the success and safety of PDT hinge on one critical factor: the force applied during the procedure.
Emerging evidence highlights how excessive dilatational force can lead to catastrophic complications. Understanding this risk and adopting refined techniques such as controlled force application and pre-dilation dissection can significantly improve outcomes.
The Role of Dilatational Force
During PDT, the tracheal stoma is dilated to insert the tracheostomy tube. This process involves the application of force, often using instruments such as the Griggs forceps or Ciaglia Blue Rhino (CBR) dilator. While straightforward in concept, the force applied during dilation is a double-edged sword:
• Low Force: Ensures controlled dilation with minimal trauma to the tracheal rings and surrounding tissue.
• Excessive Force: Risks complications such as tracheal cartilage fractures, subcutaneous emphysema, pneumothorax, or even complete tracheal rupture.
A 2019 report highlighted two real-world cases of tracheal rupture during PDT, even when performed under bronchoscopic guidance. Excessive force or the operator’s inability to identify pre-rupture signs, such as anterior-posterior tracheal wall approximation, played a significant role in these complications.
What Research Reveals About Force Management
Recent studies have quantified the forces applied during PDT, providing insights into how experience and technique influence safety:
1. Force Profiles Differ by Expertise
• Experienced surgeons applied significantly lower forces, averaging 31.3 N (mean) compared to 48.8 N for less experienced operators.
• Procedures performed by experienced surgeons showed smoother and more consistent force curves, typically with a single peak indicating controlled dilation.
• In contrast, less experienced surgeons produced inconsistent force curves with multiple peaks, indicating poor positioning and increased tissue trauma risk.
2. Force Magnitude and Moments
• Axial force (P) was the dominant force during the procedure, but bending moments (Mx, My) and torque (Mz) were higher in less experienced operators, reflecting inefficient technique and potential for injury.
• The peak axial force reached up to 88.2 N in inexperienced hands, compared to 82.8 N in experienced ones—a critical difference when dealing with fragile tracheal structures.
3. Simulations Show the Path to Improvement
• Using a strain-gauge-equipped CBR dilator, researchers demonstrated that training and feedback could significantly reduce variability and improve procedural safety.
Why Some Dissection is Necessary
Pre-dilation dissection, though not always emphasized, can reduce the resistance faced during dilation:
• Clearing Tissue Resistance: Limited pre-tracheal dissection minimizes the force required to insert the dilator, reducing stress on tracheal rings.
• Avoiding Cartilage Damage: In cases of prolonged intubation or infection, tracheal rings may weaken or become flaccid, making them more susceptible to rupture even under normal force.
Both the 2018 experimental study and real-world cases from 2019 emphasize that minor preparatory dissection can make a substantial difference in procedural outcomes.
Training and Technology: The Future of Safer PDT
The studies also highlight the role of advanced tools and structured training in preventing complications:
1. Force-Sensing Dilators:
• Devices equipped with strain gauges provide real-time feedback on the forces applied, alerting operators when they exceed safe thresholds.
• Such tools can guide less experienced surgeons toward a safer, more consistent technique.
2. Simulation-Based Training:
• Using lifelike tracheostomy simulators, operators can practice applying optimal forces and refine their skills without putting patients at risk.
• Incorporating visual or auditory feedback during simulations can further enhance learning.
3. Standardized Techniques:
• Following well-defined procedural steps, including pre-dilation assessments and controlled force application, can minimize variability and ensure adherence to safety standards.
Takeaways for Clinicians
1. Excessive Dilatational Force Leads to Complications
• Tracheal rupture, cartilage damage, and post-procedure complications like tracheal stenosis are closely linked to higher force application.
2. Experience Matters
• Skilled operators use lower, more consistent forces, reducing procedural time and complication rates.
3. Pre-Dilation Dissection Improves Outcomes
• Small dissections before dilation reduce resistance and protect fragile tracheal structures.
4. Technology and Training Are Game-Changers
• Force-monitoring tools and simulation-based training can bridge the gap for less experienced practitioners, ensuring patient safety.
Conclusion
Percutaneous dilatational tracheostomy is a vital procedure in ICU care, but its success depends on precise execution. By understanding the risks of excessive force, embracing preparatory techniques like limited dissection, and leveraging modern training tools, clinicians can make PDT safer and more effective.
As research and technology continue to evolve, the future of PDT looks promising, offering new ways to standardize practices and reduce complications. Let’s work toward a safer, more consistent approach to this life-saving procedure.
Posted in Medical | Leave a Comment »
Posted by Dr KAMAL DEEP on February 26, 2025
Posted in Medical | Leave a Comment »
Posted by Dr KAMAL DEEP on February 24, 2025
The EGDT trial, published in The New England Journal of Medicine in 2001, was a landmark study that changed the approach to early sepsis resuscitation. It introduced structured hemodynamic targets in the first 6 hours of sepsis management, leading to a significant reduction in mortality.
| Feature | Details |
|---|---|
| Full Name | Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock |
| Objective | To determine if structured hemodynamic resuscitation within the first 6 hours of sepsis improves survival compared to usual care. |
| Study Type | Single-center, randomized controlled trial (RCT), unblinded |
| Location | Henry Ford Hospital, Detroit, USA |
| Time Period | March 1997 – March 2000 |
| Number of Patients | 263 (EGDT: 130, Standard Care: 133) |
| Setting | Emergency Department (ED) – patients presenting with early severe sepsis or septic shock |
| Follow-up Duration | 60 days |
| Primary Endpoint | In-hospital mortality |
📌 Why Was EGDT Needed?
| Criteria | Details |
|---|---|
| Inclusion Criteria | – Suspected or confirmed infection – Systolic BP <90 mmHg OR Lactate ≥4 mmol/L (signs of hypoperfusion) – Identified within 6 hours of ED presentation |
| Exclusion Criteria | – Acute pulmonary edema (fluid restriction needed) – Active GI hemorrhage (requiring blood products) – DNR status, pregnancy, age <18 years – Already received >1L IV fluids before arrival |
📌 Key Point: Patients included had severe sepsis or early septic shock but had not yet received aggressive resuscitation.
| Feature | EGDT Group (Structured Resuscitation) | Standard Care Group |
|---|---|---|
| Fluids (First 6 Hours) | 30 mL/kg IV crystalloid bolus, then guided by CVP | Fluids given at clinician discretion |
| CVP Target | 8–12 mmHg | No specific target |
| MAP Target | ≥65 mmHg (fluids → vasopressors if needed) | No strict MAP goal |
| ScvO₂ Target | ≥70% (if low, added dobutamine or transfusion if Hct <30%) | Not measured |
| Urine Output Goal | ≥0.5 mL/kg/hr | No strict target |
| Vasopressors | Given if MAP <65 after fluids | Used based on clinician discretion |
| Blood Transfusion | If hematocrit <30% | Given if judged necessary |
| Dobutamine Use | If ScvO₂ <70% despite fluids | Rarely used |
📌 Why 30 mL/kg Fluids?
📌 Why ScvO₂ Monitoring?
| Parameter (First 6h) | EGDT Group | Standard Care | Difference |
|---|---|---|---|
| Total IV Fluids | 4.9L (IQR: 3.5–6.3L) | 3.5L (IQR: 2.5–5.0L) | +1.4L in EGDT |
| Blood Transfusions (%) | 19% | 4% | +15% in EGDT |
| Dobutamine Use (%) | 13.7% | 0.8% | More frequent in EGDT |
📌 EGDT patients received more fluids, blood transfusions, and inotropes than the standard care group.
| Outcome | EGDT | Standard Care | Difference |
|---|---|---|---|
| 28-Day Mortality | 30.5% | 46.5% | −16.0% (P = 0.009) |
| 60-Day Mortality | 33.3% | 49.2% | −15.9% (P = 0.01) |
📌 EGDT reduced mortality by ~16%, making it one of the most impactful sepsis trials ever conducted.
✅ EGDT proved that early, aggressive sepsis resuscitation saves lives.
✅ Hemodynamic targets (CVP, MAP, ScvO₂) improved oxygen delivery and reduced multi-organ dysfunction.
✅ A structured resuscitation protocol should begin within the first 6 hours of sepsis recognition.
🔹 Single-Center Study → Conducted only at Henry Ford Hospital (concerns about generalizability).
🔹 Control Group Received Suboptimal Care → Standard care patients may have been under-resuscitated.
🔹 ScvO₂ Monitoring is Invasive & Outdated → Later trials showed that ScvO₂ isn’t necessary for good outcomes.
🔹 PROCESS, ARISE, & PROMISE Trials (2014–2015) failed to replicate the mortality benefit → Questioning the necessity of strict EGDT protocols.
| EGDT (2001) | Modern Sepsis Management (2024) |
|---|---|
| 30 mL/kg fluids → CVP target (8–12 mmHg) | 30 mL/kg fluids → Dynamic assessment (PLR, VTI, IVC) |
| ScvO₂ monitoring with central line | Capillary refill time, lactate clearance instead |
| Dobutamine if ScvO₂ <70% | Echocardiography-based cardiac function assessment |
| Blood transfusions if Hct <30% | Less reliance on transfusions unless Hb <7 g/dL |
📌 Key Change: EGDT’s aggressive protocol is no longer required, but the concept of early, structured resuscitation remains critical.
💡 “EGDT revolutionized sepsis care by proving that aggressive early resuscitation saves lives. However, modern sepsis management has evolved, focusing on dynamic assessments rather than fixed resuscitation targets.”
Next Trial: PROCESS (2014) – The First Major Challenge to EGDT
The PROCESS (Protocolized Care for Early Septic Shock) trial, published in The New England Journal of Medicine in 2014, was the first major study to challenge EGDT. It aimed to determine whether a structured, EGDT-like approach was superior to usual care in modern sepsis management.
| Feature | Details |
|---|---|
| Full Name | Protocolized Care for Early Septic Shock (PROCESS) |
| Objective | To compare EGDT vs. protocolized resuscitation vs. usual care in early septic shock |
| Study Type | Multicenter, RCT, unblinded, noninferiority trial |
| Location | 31 centers (USA) |
| Time Period | March 2008 – May 2013 |
| Number of Patients | 1,341 |
| Setting | Emergency Departments (ED) – patients presenting with early septic shock |
| Follow-up Duration | 60 days |
| Primary Endpoint | 60-day mortality |
📌 Why Was PROCESS Needed?
| Criteria | Details |
|---|---|
| Inclusion Criteria | – Suspected infection + lactate ≥4 mmol/L OR persistent hypotension after 1L fluids – Must be randomized within 2 hours of meeting criteria |
| Exclusion Criteria | – DNR status, pregnancy, acute pulmonary edema, active bleeding – >2L fluids already given before randomization |
📌 Key Difference from EGDT: Patients were enrolled within 2 hours (EGDT allowed 6 hours).
| Feature | EGDT (Rivers’ Protocol) | Protocolized Standard Care | Usual Care |
|---|---|---|---|
| Fluids (First 6 Hours) | 30 mL/kg IV crystalloid (CVP-guided) | 30 mL/kg IV crystalloid (MAP-guided) | Fluids given at clinician’s discretion |
| Vasopressors | MAP goal ≥65 mmHg | MAP goal ≥65 mmHg | Used if necessary |
| ScvO₂ Target | ≥70% (via CVC monitoring) | Not required | Not required |
| Dobutamine Use | If ScvO₂ <70% | Rarely used | Rarely used |
| Blood Transfusion | Hematocrit <30% | Hb <7 g/dL | Hb <7 g/dL |
📌 Key Difference from EGDT: The protocolized standard care group received the same volume of fluids but without invasive ScvO₂ monitoring.
| Parameter (First 6h) | EGDT Group | Protocolized Care | Usual Care |
|---|---|---|---|
| Total IV Fluids | 4.9L | 3.9L | 3.3L |
| Vasopressors Use (%) | 54.9% | 52.2% | 44.1% |
| Dobutamine Use (%) | 8.0% | 1.1% | 0.9% |
| Blood Transfusion (%) | 14.4% | 8.3% | 7.5% |
📌 Key Findings:
| Outcome | EGDT | Protocolized Care | Usual Care | Difference |
|---|---|---|---|---|
| 60-Day Mortality | 21.0% | 18.2% | 18.9% | No significant difference (P = 0.83) |
| 90-Day Mortality | 31.9% | 30.9% | 34.0% | No significant difference (P = 0.61) |
📌 Key Takeaway: EGDT did not improve survival compared to modern usual care.
✅ EGDT’s structured protocol is not superior to modern usual care.
✅ Early fluids (30 mL/kg) and MAP-guided resuscitation work just as well without ScvO₂ monitoring.
✅ Routine blood transfusions and dobutamine use are unnecessary.
📌 PROCESS showed that modern sepsis care already includes aggressive early resuscitation, making EGDT redundant.
🔹 Unblinded Study → Clinicians knew which group patients were in, which may have influenced treatment.
🔹 Better Overall Sepsis Care → The control group received early antibiotics and fluid resuscitation, unlike the original EGDT trial in 2001.
🔹 Generalizability to Low-Resource Settings? → EGDT might still benefit hospitals without strong sepsis protocols.
| Feature | EGDT (2001) | PROCESS (2014) |
|---|---|---|
| Required ScvO₂ Monitoring? | Yes (central line needed) | No (not necessary) |
| Fluids Given? | 30 mL/kg guided by CVP | 30 mL/kg guided by MAP |
| Vasopressor Use? | Only after fluids | Started earlier if MAP <65 |
| Blood Transfusion? | Hct <30% | Hb <7 g/dL |
| Mortality Benefit? | Yes (16% reduction) | No difference |
📌 Key Change: EGDT’s invasive monitoring and strict protocol were unnecessary when sepsis care improved overall.
💡 “PROCESS proved that modern sepsis care (early antibiotics, MAP-guided fluids, and vasopressors) is just as effective as EGDT. The key takeaway? We don’t need central line-driven ScvO₂ monitoring or rigid protocols anymore—what matters most is early resuscitation and individualized fluid management.”
The ARISE (Australasian Resuscitation in Sepsis Evaluation) trial, published in The New England Journal of Medicine in 2014, was a large, multicenter, randomized controlled trial (RCT) designed to determine whether EGDT was superior to modern usual care in early septic shock. It was conducted simultaneously with the PROCESS trial and confirmed that EGDT is not necessary for good outcomes when early antibiotics and fluid resuscitation are provided.
| Feature | Details |
|---|---|
| Full Name | Australasian Resuscitation in Sepsis Evaluation (ARISE) |
| Objective | To determine whether EGDT improves survival compared to usual care in early septic shock |
| Study Type | Multicenter, RCT, unblinded, noninferiority trial |
| Location | 51 centers (Australia, New Zealand, Finland, Hong Kong, Ireland, UK) |
| Time Period | October 2008 – April 2014 |
| Number of Patients | 1,600 |
| Setting | Emergency Departments (ED) – patients presenting with early septic shock |
| Follow-up Duration | 90 days |
| Primary Endpoint | 90-day all-cause mortality |
📌 Why Was ARISE Needed?
| Criteria | Details |
|---|---|
| Inclusion Criteria | – Suspected or confirmed infection – Lactate ≥4 mmol/L OR persistent hypotension (MAP <65) after 1L IV fluids – Must be randomized within 6 hours of ED presentation |
| Exclusion Criteria | – DNR status, pregnancy, acute pulmonary edema, active GI bleeding – >1L IV fluids already given before randomization |
📌 Key Difference from PROCESS:
| Feature | EGDT (Rivers’ Protocol) | Usual Care |
|---|---|---|
| Fluids (First 6 Hours) | 30 mL/kg IV crystalloid (CVP-guided) | Fluids given at clinician’s discretion |
| Vasopressors | MAP goal ≥65 mmHg | MAP goal ≥65 mmHg |
| ScvO₂ Monitoring | Yes (≥70%) | Not required |
| Dobutamine Use | If ScvO₂ <70% | Rarely used |
| Blood Transfusion | Hematocrit <30% | Hb <7 g/dL |
📌 Key Difference from EGDT (2001):
| Parameter (First 6h) | EGDT Group | Usual Care | Difference |
|---|---|---|---|
| Total IV Fluids | 4.3L | 4.0L | Not significantly different |
| Vasopressors Use (%) | 76.3% | 67.7% | Slightly more in EGDT group |
| Dobutamine Use (%) | 15.4% | 2.6% | More in EGDT group |
| Blood Transfusion (%) | 13.6% | 7.0% | More in EGDT group |
📌 Key Findings:
| Outcome | EGDT | Usual Care | Difference |
|---|---|---|---|
| 90-Day Mortality | 18.6% | 18.8% | No significant difference (P = 0.90) |
| ICU-Free Days | 14.3 days | 14.0 days | No significant difference |
| Ventilator-Free Days | 19.5 days | 19.6 days | No significant difference |
📌 Key Takeaway: EGDT did not improve survival compared to modern usual care.
✅ EGDT’s structured protocol is not superior to modern usual care.
✅ Early antibiotics, aggressive resuscitation, and MAP-guided fluids work just as well.
✅ Routine blood transfusions and dobutamine use are unnecessary.
📌 ARISE confirmed what PROCESS had already shown: EGDT is not needed when early sepsis care is optimized.
🔹 Unblinded Study → Clinicians knew which group patients were in, which could introduce bias.
🔹 Better Overall Sepsis Care → The control group received early antibiotics and fluid resuscitation, unlike in 2001 when EGDT was first introduced.
🔹 Does This Apply to Low-Resource Settings? → EGDT might still help in hospitals without strong sepsis protocols.
| Feature | EGDT (2001) | ARISE (2014) |
|---|---|---|
| Required ScvO₂ Monitoring? | Yes (central line needed) | No (not necessary) |
| Fluids Given? | 30 mL/kg guided by CVP | 30 mL/kg guided by MAP |
| Vasopressor Use? | Only after fluids | Started earlier if MAP <65 |
| Blood Transfusion? | Hct <30% | Hb <7 g/dL |
| Mortality Benefit? | Yes (16% reduction in 2001) | No difference in 2014 |
📌 Key Change: EGDT’s invasive monitoring and strict protocol were unnecessary when sepsis care improved overall.
💡 “ARISE confirmed that modern sepsis care (early antibiotics, MAP-guided fluids, and vasopressors) is just as effective as EGDT. The key takeaway? We don’t need central line-driven ScvO₂ monitoring or rigid protocols anymore—what matters most is early resuscitation and individualized fluid management.”
The PROMISE (Protocolized Management in Sepsis) trial, published in The New England Journal of Medicine in 2015, was the third major study—after PROCESS and ARISE—to test whether EGDT improved survival over usual care in early septic shock. Like its predecessors, PROMISE found no survival benefit with EGDT, further cementing the idea that modern sepsis care (early antibiotics, fluid resuscitation, vasopressors) was already optimized without the need for EGDT’s strict protocol.
| Feature | Details |
|---|---|
| Full Name | Protocolized Management in Sepsis (PROMISE) |
| Objective | To determine whether EGDT improves survival compared to usual care in early septic shock |
| Study Type | Multicenter, RCT, unblinded, noninferiority trial |
| Location | 56 centers (United Kingdom) |
| Time Period | February 2011 – July 2014 |
| Number of Patients | 1,260 |
| Setting | Emergency Departments (ED) – patients presenting with early septic shock |
| Follow-up Duration | 90 days |
| Primary Endpoint | 90-day all-cause mortality |
📌 Why Was PROMISE Needed?
| Criteria | Details |
|---|---|
| Inclusion Criteria | – Suspected infection + lactate ≥4 mmol/L OR persistent hypotension (MAP <65) after 1L IV fluids – Must be randomized within 6 hours of ED presentation |
| Exclusion Criteria | – DNR status, pregnancy, acute pulmonary edema, active GI bleeding – >1L IV fluids already given before randomization |
📌 Key Similarity to ARISE:
| Feature | EGDT (Rivers’ Protocol) | Usual Care |
|---|---|---|
| Fluids (First 6 Hours) | 30 mL/kg IV crystalloid (CVP-guided) | Fluids given at clinician’s discretion |
| Vasopressors | MAP goal ≥65 mmHg | MAP goal ≥65 mmHg |
| ScvO₂ Monitoring | Yes (≥70%) | Not required |
| Dobutamine Use | If ScvO₂ <70% | Rarely used |
| Blood Transfusion | Hematocrit <30% | Hb <7 g/dL |
📌 Key Similarity to PROCESS & ARISE:
| Parameter (First 6h) | EGDT Group | Usual Care | Difference |
|---|---|---|---|
| Total IV Fluids | 4.0L | 3.9L | Not significantly different |
| Vasopressors Use (%) | 53.7% | 46.6% | Slightly more in EGDT group |
| Dobutamine Use (%) | 8.0% | 2.6% | More in EGDT group |
| Blood Transfusion (%) | 8.9% | 7.0% | More in EGDT group |
📌 Key Findings:
| Outcome | EGDT | Usual Care | Difference |
|---|---|---|---|
| 90-Day Mortality | 29.5% | 29.2% | No significant difference (P = 0.90) |
| ICU-Free Days | 13.5 days | 13.0 days | No significant difference |
| Ventilator-Free Days | 18.2 days | 18.1 days | No significant difference |
📌 Key Takeaway: EGDT did not improve survival compared to modern usual care.
✅ EGDT’s structured protocol is not superior to modern usual care.
✅ Early antibiotics, aggressive resuscitation, and MAP-guided fluids work just as well.
✅ Routine blood transfusions and dobutamine use are unnecessary.
📌 PROMISE confirmed the findings of PROCESS & ARISE: EGDT is not needed when early sepsis care is optimized.
🔹 Unblinded Study → Clinicians knew which group patients were in, which could introduce bias.
🔹 Better Overall Sepsis Care → The control group received early antibiotics and fluid resuscitation, unlike in 2001 when EGDT was first introduced.
🔹 Does This Apply to Low-Resource Settings? → EGDT might still help in hospitals without strong sepsis protocols.
| Feature | EGDT (2001) | PROMISE (2015) |
|---|---|---|
| Required ScvO₂ Monitoring? | Yes (central line needed) | No (not necessary) |
| Fluids Given? | 30 mL/kg guided by CVP | 30 mL/kg guided by MAP |
| Vasopressor Use? | Only after fluids | Started earlier if MAP <65 |
| Blood Transfusion? | Hct <30% | Hb <7 g/dL |
| Mortality Benefit? | Yes (16% reduction in 2001) | No difference in 2015 |
📌 Key Change: EGDT’s invasive monitoring and strict protocol were unnecessary when sepsis care improved overall.
💡 “PROMISE was the final nail in EGDT’s coffin. It confirmed what PROCESS and ARISE already showed—early antibiotics, MAP-guided fluids, and vasopressors are just as effective as EGDT’s rigid protocol. Today, we focus on individualized resuscitation rather than fixed targets like ScvO₂ and CVP.”
The CLASSIC (Conservative vs. Liberal Approach to Fluid Therapy in Septic Shock in Intensive Care) trial, published in The New England Journal of Medicine in 2022, was a large, multicenter, randomized controlled trial (RCT) designed to determine whether a restrictive IV fluid strategy improves survival compared to standard (liberal) fluid administration in patients with septic shock in the ICU.
Key Finding: The trial found no significant difference in mortality between restrictive and liberal fluids, suggesting that fluid restriction after initial resuscitation does not improve survival in septic shock.
| Feature | Details |
|---|---|
| Full Name | Conservative vs. Liberal Approach to Fluid Therapy in Septic Shock in Intensive Care (CLASSIC) |
| Objective | To compare restrictive IV fluids vs. usual-care fluid therapy in ICU patients with septic shock |
| Study Type | Multicenter, RCT, open-label |
| Location | 31 ICUs (Denmark, Norway, Sweden, Finland, Switzerland, the UK, and Belgium) |
| Time Period | December 2018 – September 2021 |
| Number of Patients | 1,554 |
| Setting | ICU patients with septic shock who had already received initial fluid resuscitation |
| Follow-up Duration | 90 days |
| Primary Endpoint | 90-day all-cause mortality |
📌 Why Was CLASSIC Needed?
📌 Key Difference from CLOVERS:
| Criteria | Details |
|---|---|
| Inclusion Criteria | – Septic shock requiring vasopressors for ≥1 hour – Received at least 1L IV fluids before enrollment – Randomization within 12 hours of septic shock onset |
| Exclusion Criteria | – Septic shock duration >12 hours – Major bleeding, acute burns, pregnancy, severe dehydration – ICU admission for non-sepsis reasons |
📌 Key Difference from CLOVERS: CLASSIC excluded patients in the early resuscitation phase and focused on post-resuscitation fluid management.
| Feature | Restrictive Fluid Strategy | Standard Fluid Strategy (Liberal Fluids) |
|---|---|---|
| Fluids Post-Randomization | Minimal fluids unless clear need | Fluids given per standard ICU practice |
| Fluid Triggers | Fluids only for severe hypoperfusion, oliguria, or marked fluid loss | Fluids given at clinician discretion |
| Vasopressor Use | Earlier vasopressors instead of fluids | Fluids first, then vasopressors if needed |
| Rescue Fluids | Allowed if lactate >4 mmol/L, MAP <50, or ScvO₂ <65% | Fluids given more liberally |
| Monitoring | Dynamic assessments | CVP, lactate, bedside clinical signs |
📌 Key Difference from CLOVERS: CLASSIC patients were already in septic shock (on vasopressors), while CLOVERS tested early vasopressors vs. liberal fluids in sepsis-induced hypotension.
| Parameter (First 24h Post-Randomization) | Restrictive Group | Standard Care Group | Difference |
|---|---|---|---|
| Total IV Fluids (First 24h) | 1,798 mL (IQR: 500–3,000 mL) | 2,980 mL (IQR: 1,998–4,000 mL) | -1,182 mL less in restrictive group |
| Cumulative Fluids (First 5 Days) | 1,798 mL | 3,811 mL | -2,013 mL less in restrictive group |
| Vasopressor Use (%) | 100% (all required vasopressors at enrollment) | 100% | No difference |
📌 Key Findings:
| Outcome | Restrictive Fluids | Standard Fluids | Difference |
|---|---|---|---|
| 90-Day Mortality | 42.3% | 42.1% | No significant difference (P = 0.96) |
| 28-Day Mortality | 34.5% | 34.2% | No difference |
📌 Key Takeaway: Restricting fluids did not improve survival in ICU septic shock.
| Outcome | Restrictive Fluids | Standard Fluids | P-Value |
|---|---|---|---|
| Days Alive Without Life Support (Day 90) | 47 days | 47 days | NS |
| Days Alive and Out of Hospital (Day 90) | 33 days | 34 days | NS |
| Serious Adverse Events | No significant difference | No significant difference | NS |
📌 Key Takeaway: Fluid restriction did not reduce ventilator days, organ failure, or hospital stay.
✅ Restricting fluids after ICU admission does not improve survival in septic shock.
✅ Early vasopressors do not necessarily reduce mortality.
✅ Fluids should be guided by individual patient needs rather than rigid protocols.
📌 CLASSIC suggests that a restrictive approach is not superior to usual-care fluids. Instead, individualized fluid resuscitation is key.
🔹 Open-Label Study → Clinicians knew which group patients were in, introducing potential bias.
🔹 Exclusion of Severe Hypovolemia → Patients with dehydration or severe fluid losses were excluded, limiting generalizability.
🔹 Did Not Study Early Sepsis → CLASSIC focused on ICU septic shock, not early sepsis (like CLOVERS).
| Feature | CLASSIC (2022) | CLOVERS (2023) |
|---|---|---|
| Setting | ICU patients already in septic shock | Early sepsis in ED/Wards |
| Intervention | Restrictive fluids vs. usual fluids (ICU phase) | Early vasopressors vs. liberal fluids (initial resuscitation) |
| Key Finding | No survival benefit of fluid restriction | No survival difference between early vasopressors & liberal fluids |
📌 Key Takeaway: CLASSIC and CLOVERS both show that fluid strategy matters less than individualized resuscitation based on patient response.
💡 “CLASSIC showed that restrictive fluids do not improve survival in ICU septic shock. The key takeaway? Individualized fluid management is more important than strict liberal or restrictive strategies.”
The CLOVERS (Crystalloid Liberal or Vasopressors Early Resuscitation in Sepsis) trial, published in The New England Journal of Medicine in 2023, investigated whether an early vasopressor strategy with restricted fluids improves outcomes compared to a liberal fluid strategy in patients with sepsis-induced hypotension.
Key Finding: There was no difference in 90-day mortality between early vasopressors and liberal fluids, suggesting no clear advantage of restricting fluids and starting vasopressors early.
| Feature | Details |
|---|---|
| Full Name | Crystalloid Liberal or Vasopressors Early Resuscitation in Sepsis (CLOVERS) |
| Objective | To compare early vasopressors with restrictive fluids vs. liberal IV fluids in early sepsis-induced hypotension |
| Study Type | Multicenter, RCT, unblinded |
| Location | 60 centers (USA, National Heart, Lung, and Blood Institute) |
| Time Period | March 2018 – January 2022 |
| Number of Patients | 1,563 |
| Setting | Emergency Department (ED) and hospital wards – early sepsis before ICU admission |
| Follow-up Duration | 90 days |
| Primary Endpoint | 90-day all-cause mortality |
📌 Why Was CLOVERS Needed?
📌 Key Difference from CLASSIC (2022):
| Criteria | Details |
|---|---|
| Inclusion Criteria | – Sepsis-induced hypotension (MAP <65 mmHg or SBP <100 mmHg) after 1–3L IV fluids – Suspected or confirmed infection – Randomization within 4 hours of meeting criteria |
| Exclusion Criteria | – Septic shock requiring immediate ICU admission – Severe volume depletion (e.g., GI bleed, pancreatitis) – Active hemorrhage, pregnancy, cardiac arrest, CHF, ESRD on dialysis |
📌 Key Inclusion Criteria: Patients were early in sepsis, before ICU admission, with persistent hypotension despite 1–3L IV fluids.
📌 Key Exclusion: Patients already in septic shock (requiring immediate ICU care) were excluded.
| Feature | Restrictive Fluids (Early Vasopressors) | Liberal Fluids Strategy |
|---|---|---|
| Fluids Post-Randomization | Minimal fluids unless severe hypoperfusion | Aggressive fluid resuscitation (goal 30 mL/kg) |
| Vasopressors | Early norepinephrine infusion if MAP <65 | Started only if fluids failed to restore MAP |
| Fluid Rescue Triggers | Fluids only for lactate >4 mmol/L, severe oliguria, persistent shock | Fluids given as first-line therapy |
| Monitoring | Frequent reassessment for tissue perfusion | Fluids given until perfusion improved |
📌 Key Difference from CLASSIC:
| Parameter (First 24h Post-Randomization) | Restrictive (Early Vasopressors) | Liberal Fluids | Difference |
|---|---|---|---|
| Total IV Fluids (First 24h) | 1267 mL (IQR: 555–2279 mL) | 3400 mL (IQR: 2500–4495 mL) | -2,133 mL less in restrictive group |
| Cumulative Fluids (First 5 Days) | 3300 mL | 5400 mL | -2,100 mL less in restrictive group |
| Vasopressor Use (%) | 59% | 37% | Earlier and more common in restrictive group |
📌 Key Findings:
| Outcome | Restrictive Fluids | Liberal Fluids | Difference |
|---|---|---|---|
| 90-Day Mortality | 14.0% | 14.9% | No significant difference (P = 0.61) |
| 28-Day Mortality | 10.3% | 11.3% | No significant difference |
📌 Key Takeaway: Restricting fluids and using early vasopressors did not improve survival in early sepsis.
| Outcome | Restrictive Fluids | Liberal Fluids | P-Value |
|---|---|---|---|
| Days Free from Organ Support (Day 28) | 21 days | 21 days | NS |
| Ventilator-Free Days | 23.4 days | 22.8 days | NS |
| ICU Length of Stay | 6.5 days | 6.7 days | NS |
| Serious Adverse Events | 10.6% | 10.5% | NS |
📌 Key Takeaway: No difference in ventilator days, ICU stay, or organ failure between groups.
✅ Restricting fluids in early sepsis does not improve survival.
✅ Early vasopressors are safe but offer no mortality benefit over liberal fluids.
✅ Sepsis resuscitation should be individualized rather than following rigid protocols.
📌 CLOVERS suggests that both fluid-first and early vasopressor-first approaches are reasonable, emphasizing the need for individualized resuscitation.
🔹 Unblinded Study → Clinicians knew which group patients were in, introducing potential bias.
🔹 Excluded ICU Septic Shock Patients → Results do not apply to patients already in severe septic shock.
🔹 Low Vasopressor Use in Restrictive Group → Only 59% received vasopressors, raising concerns about protocol adherence.
| Feature | CLOVERS (2023) | CLASSIC (2022) |
|---|---|---|
| Setting | Early sepsis (ED/Wards, pre-ICU) | Septic shock (ICU, post-resuscitation) |
| Intervention | Restrictive fluids with early vasopressors vs. liberal fluids | Restrictive fluids vs. usual fluids |
| Key Finding | No survival difference between fluid-first and vasopressor-first | No survival benefit of fluid restriction in ICU septic shock |
📌 Key Takeaway: Both trials emphasize individualized fluid management over rigid strategies.
💡 “CLOVERS showed that early vasopressors are not superior to liberal fluids in early sepsis resuscitation. The key takeaway? Sepsis resuscitation should be individualized, balancing fluids and vasopressors based on patient needs.”
The FACTT (Fluid and Catheter Treatment Trial), published in The New England Journal of Medicine in 2006, was a landmark study that investigated whether a liberal or conservative fluid strategy improved outcomes in patients with acute respiratory distress syndrome (ARDS).
Key Finding: A conservative fluid strategy improved lung function, reduced ventilator days, and shortened ICU stays—without increasing shock or worsening organ perfusion.
| Feature | Details |
|---|---|
| Full Name | Fluid and Catheter Treatment Trial (FACTT) |
| Objective | To compare liberal vs. conservative fluid management strategies in ARDS |
| Study Type | Multicenter, RCT, 2×2 factorial design |
| Location | 20 ARDS Network hospitals (USA) |
| Time Period | June 2000 – October 2005 |
| Number of Patients | 1,000 |
| Setting | ICU patients with ARDS (ventilated) |
| Follow-up Duration | 60 days |
| Primary Endpoint | 60-day mortality |
📌 Why Was FACTT Needed?
📌 Key Unique Feature:
| Criteria | Details |
|---|---|
| Inclusion Criteria | – ARDS diagnosis (PaO₂/FiO₂ ≤ 300 mmHg, bilateral infiltrates, non-cardiogenic cause) – Mechanical ventilation required – Randomization within 48 hours of ARDS onset |
| Exclusion Criteria | – Severe CHF, chronic lung disease, CKD, cirrhosis – High risk of volume depletion (GI bleeding, acute pancreatitis) |
📌 Key Inclusion: Patients had confirmed ARDS and required ventilation.
📌 Key Exclusion: Severe CHF and CKD patients were excluded to avoid confounding due to volume status.
| Feature | Conservative Fluids | Liberal Fluids |
|---|---|---|
| Daily Fluid Goal | Maintain CVP <4 mmHg | Maintain CVP 10–14 mmHg |
| Diuretic Use | Aggressive diuresis allowed | Minimal diuretics |
| Vasopressor Use | Allowed if needed to maintain MAP | Fluids first, then vasopressors if needed |
| Monitoring | CVP or PA catheter to guide fluids | Same |
📌 Key Difference: The conservative group received fewer fluids and more diuretics to actively remove excess fluid, while the liberal group received fluids to maintain higher CVP.
| Parameter (First 7 Days Post-Randomization) | Conservative Fluids | Liberal Fluids | Difference |
|---|---|---|---|
| Total IV Fluids (7 days) | 1.0L (median) | 7.0L (median) | -6.0L less in conservative group |
| Fluid Balance (7 days) | -136 mL (net fluid loss) | +6,992 mL (net fluid gain) | ~7L difference |
| Diuretic Use (%) | 68% | 21% | More frequent in conservative group |
| Vasopressor Use (%) | 66% | 57% | Slightly more in conservative group |
📌 Key Findings:
| Outcome | Conservative Fluids | Liberal Fluids | Difference |
|---|---|---|---|
| 60-Day Mortality | 25.5% | 28.4% | No significant difference (P = 0.30) |
| ICU Mortality | 16.9% | 19.7% | No significant difference |
📌 Key Takeaway: Conservative fluids did NOT reduce mortality compared to liberal fluids.
| Outcome | Conservative Fluids | Liberal Fluids | P-Value |
|---|---|---|---|
| Ventilator-Free Days (Day 28) | 14.6 days | 12.1 days | P < 0.001 |
| ICU-Free Days (Day 28) | 13.4 days | 11.2 days | P < 0.001 |
| Oxygenation (PaO₂/FiO₂ at Day 7) | +23 mmHg improvement | No significant change | P < 0.001 |
| Acute Kidney Injury (AKI) | 10% | 14% | P < 0.05 (fewer AKI in conservative group) |
📌 Key Takeaway: Conservative fluids improved lung function, reduced ventilator days, and lowered ICU stay without increasing AKI.
✅ A conservative fluid strategy improves lung function and shortens ICU stay in ARDS.
✅ Conservative fluids reduce ventilator days without harming circulation.
✅ Excess fluids worsen lung function, oxygenation, and ICU outcomes.
📌 FACTT changed ARDS management by promoting conservative fluids and diuresis.
🔹 Did Not Assess Long-Term Outcomes → Follow-up was limited to 60 days.
🔹 Excluded Severe Hypovolemia → Results may not apply to septic shock patients needing aggressive fluids.
🔹 Higher Vasopressor Use in Conservative Group → More patients required vasopressors, though this did not worsen mortality.
| Feature | FACTT (2006) | CLOVERS (2023) | CLASSIC (2022) |
|---|---|---|---|
| Setting | ICU patients with ARDS | Early sepsis (ED/Wards) | ICU septic shock |
| Intervention | Restrictive vs. Liberal fluids in ARDS | Early vasopressors vs. fluids in sepsis | Restrictive vs. usual fluids in septic shock |
| Key Finding | Restrictive fluids improved lung function & reduced ICU stay | No survival benefit of early vasopressors | No survival benefit of fluid restriction |
📌 Key Takeaway: FACTT supports conservative fluids in ARDS, while CLOVERS & CLASSIC suggest individualized fluid management in sepsis.
💡 “FACTT revolutionized ARDS management by proving that conservative fluid strategies improve lung function, reduce ventilator days, and shorten ICU stay—without increasing mortality. The key takeaway? Avoid fluid overload in ARDS and use diuresis when needed.”
The ANDROMEDA-SHOCK trial, published in JAMA in 2019, was a multicenter randomized controlled trial (RCT) designed to compare capillary refill time (CRT)-guided resuscitation vs. lactate clearance-guided resuscitation in patients with septic shock.
Key Finding: CRT-guided resuscitation led to less fluid administration and faster resolution of shock, without increasing mortality.
| Feature | Details |
|---|---|
| Full Name | ANDROMEDA-SHOCK (ANDROmeda Sepsis SHOCK) |
| Objective | To compare capillary refill time (CRT) vs. lactate clearance for guiding fluid resuscitation in septic shock |
| Study Type | Multicenter, RCT, open-label |
| Location | 28 ICUs (Argentina, Chile, Colombia, Ecuador, Uruguay) |
| Time Period | March 2017 – March 2018 |
| Number of Patients | 424 |
| Setting | ICU patients with septic shock |
| Follow-up Duration | 28 days |
| Primary Endpoint | 28-day all-cause mortality |
📌 Why Was ANDROMEDA-SHOCK Needed?
📌 Key Novel Feature:
| Criteria | Details |
|---|---|
| Inclusion Criteria | – Septic shock requiring vasopressors after ≥20 mL/kg IV fluids – Lactate ≥2 mmol/L |
| Exclusion Criteria | – Acute hemorrhage, severe trauma, acute pulmonary edema, DNR status – Severe liver failure (Child-Pugh C), chronic kidney disease (CKD), pregnancy |
📌 Key Inclusion: Patients had persistent septic shock despite initial fluid resuscitation.
📌 Key Exclusion: Conditions where CRT or lactate might be unreliable (e.g., liver failure, acute bleeding).
| Feature | CRT-Guided Resuscitation | Lactate-Guided Resuscitation |
|---|---|---|
| Perfusion Target | CRT ≤3 seconds | Lactate decrease by ≥20% every 2 hours |
| Fluids (After Randomization) | Fluids stopped if CRT normalized | Fluids continued if lactate remained high |
| Vasopressor Use | Adjusted based on CRT response | Adjusted based on lactate response |
| Monitoring | Reassessed every 30 minutes | Lactate rechecked every 2 hours |
📌 Key Difference: CRT was reassessed every 30 minutes (fast response), while lactate took longer (every 2 hours).
| Parameter (First 8h Post-Randomization) | CRT-Guided Group | Lactate-Guided Group | Difference |
|---|---|---|---|
| Total IV Fluids (8h) | 1.4L (IQR: 0.9–2.1L) | 1.8L (IQR: 1.2–2.6L) | -400 mL less in CRT group |
| Cumulative Fluids (First 24h) | 2.4L | 3.2L | -800 mL less in CRT group |
| Vasopressor Use (%) | Higher in CRT group (faster escalation to norepinephrine) | Delayed vasopressors in lactate group |
📌 Key Findings:
| Outcome | CRT-Guided Resuscitation | Lactate-Guided Resuscitation | Difference |
|---|---|---|---|
| 28-Day Mortality | 34.9% | 43.4% | No significant difference (P = 0.06) |
📌 Key Takeaway: CRT-guided resuscitation did not significantly reduce mortality, but there was a trend toward benefit (P = 0.06).
| Outcome | CRT-Guided Resuscitation | Lactate-Guided Resuscitation | P-Value |
|---|---|---|---|
| Organ Failure-Free Days | 14.5 days | 13.0 days | P = 0.045 |
| ICU-Free Days | 10.0 days | 8.5 days | P = 0.04 |
| Vasopressor-Free Days | 17.0 days | 15.0 days | P = 0.04 |
| Ventilator-Free Days | 16.5 days | 14.0 days | P = 0.03 |
📌 Key Takeaway: CRT-guided resuscitation led to faster shock resolution, fewer organ failures, and earlier ICU discharge.
✅ CRT is a simple bedside tool that rapidly reflects tissue perfusion.
✅ CRT-guided resuscitation reduced fluid administration and improved organ recovery.
✅ Lactate clearance alone may lead to excessive fluid resuscitation.
📌 ANDROMEDA-SHOCK suggests that CRT should be included in septic shock resuscitation strategies.
🔹 Underpowered for Mortality → The trial was not powered to detect mortality differences (P = 0.06 trend toward CRT benefit).
🔹 Open-Label Design → Clinicians knew the resuscitation strategy, potentially influencing decisions.
🔹 Excluded Severe Hypovolemia → Results may not apply to patients needing aggressive volume resuscitation.
| Feature | ANDROMEDA-SHOCK (2019) | PROCESS (2014) | ARISE (2014) | PROMISE (2015) |
|---|---|---|---|---|
| Setting | ICU patients with septic shock | Early sepsis (ED/Wards) | Early sepsis (ED/Wards) | Early sepsis (ED/Wards) |
| Intervention | CRT vs. lactate for resuscitation | EGDT vs. usual care | EGDT vs. usual care | EGDT vs. usual care |
| Key Finding | CRT led to faster shock resolution with less fluids | EGDT not superior to usual care | EGDT not superior to usual care | EGDT not superior to usual care |
📌 Key Takeaway: ANDROMEDA-SHOCK showed that CRT is a fast, effective bedside tool for guiding resuscitation, while prior sepsis trials focused on structured protocols vs. usual care.
💡 “ANDROMEDA-SHOCK proved that capillary refill time is a simple, rapid, and effective bedside tool for resuscitation in septic shock. CRT-guided resuscitation reduces fluid overload and improves organ recovery—without compromising perfusion.”
Both CLOVERS (2023) and CLASSIC (2022) are major randomized controlled trials that investigated restrictive vs. liberal fluid resuscitation strategies in septic shock. However, they differ in patient population, timing of intervention, volume of fluids given, and outcomes.
| Feature | CLOVERS Trial (2023) | CLASSIC Trial (2022) |
|---|---|---|
| Full Name | Crystalloid Liberal or Vasopressors Early Resuscitation in Sepsis | Conservative vs. Liberal Approach to Fluid Therapy in Septic Shock |
| Objective | Early resuscitation: Compare restrictive (early vasopressors) vs. liberal (more fluids) approach in sepsis-induced hypotension | ICU fluid management: Compare restrictive vs. standard care in septic shock patients already admitted to the ICU |
| Study Type | Multicenter, RCT, open-label | Multicenter, RCT, open-label |
| Location | 60 centers (USA) | 31 ICUs (Europe) |
| Patients Included | Sepsis-induced hypotension (early phase, pre-ICU) | Septic shock in ICU (post-initial resuscitation phase) |
| Timing of Intervention | Early septic shock (ED & wards, within 4h of meeting criteria) | Late septic shock (ICU, after initial resuscitation) |
| Primary Hypothesis | Early vasopressors with restrictive fluids improves survival | Restricting fluids after ICU admission improves survival |
🔹 Key Difference:
| Feature | CLOVERS | CLASSIC |
|---|---|---|
| Inclusion Criteria | Suspected infection + hypotension after 1–3L fluids (MAP <65 mmHg, SBP <100 mmHg) | Septic shock requiring vasopressors after receiving ≥1L of IV fluids |
| Exclusion Criteria | >4h since hypotension, >3L fluids given, severe fluid overload, pregnancy | >12h septic shock, >4L fluids before enrollment, major bleeding, severe burns |
🔹 Key Difference:
| Feature | CLOVERS | CLASSIC |
|---|---|---|
| Restrictive Fluids Group | – Fluids limited after initial 1–3L – Early vasopressors started to maintain MAP | – Fluids minimized after ICU admission – Additional fluids given only if signs of hypoperfusion |
| Liberal/Standard Fluids Group | – Initial 2L fluid bolus, then fluids as needed – Vasopressors started only if fluids failed | – Fluids given at clinician discretion (standard ICU practice) |
🔹 Key Difference:
| Feature | CLOVERS Restrictive | CLOVERS Liberal | CLASSIC Restrictive | CLASSIC Standard |
|---|---|---|---|---|
| Fluids in First 6h | 500 mL (IQR: 130–1097) | 2300 mL (IQR: 2000–3000) | 1798 mL (IQR: 500–3000) | 2980 mL (IQR: 1998–4000) |
| Fluids in First 24h | 1267 mL (IQR: 555–2279) | 3400 mL (IQR: 2500–4495) | 1798 mL (IQR: 500–3000) | 2980 mL (IQR: 1998–4000) |
| Total Fluids (including pre-trial fluids) | 3300 mL | 5400 mL | 4900 mL | 5700 mL |
| Vasopressor Use | 59% | 37% | 100% (all required vasopressors at enrollment) | 100% |
🔹 Key Difference:
| Outcome | CLOVERS Restrictive | CLOVERS Liberal | CLASSIC Restrictive | CLASSIC Standard |
|---|---|---|---|---|
| 90-Day Mortality | 14.0% | 14.9% | 42.3% | 42.1% |
| Ventilator-Free Days | 23.4 days | 22.8 days | 19.3 days | 19.5 days |
| ICU-Free Days (28d) | 22.8 days | 22.7 days | 12.5 days | 13.0 days |
| RRT Use | 3.3% | 3.3% | 22.5% | 20.8% |
| Serious Adverse Events | 10.6% | 10.5% | No difference |
🔹 Key Takeaways:
✅ Restricting fluids does not improve survival.
✅ Liberal fluids do not significantly increase harm.
✅ Early vasopressors are safe but not clearly superior.
✅ Both trials suggest that individualized fluid management is the best approach.
🔹 CLOVERS tested early resuscitation (first few hours), CLASSIC tested ICU patients post-resuscitation.
🔹 CLOVERS tested early vasopressors vs. fluids, CLASSIC tested post-resuscitation fluid restriction.
🔹 CLOVERS patients received less fluid overall; CLASSIC patients were already on vasopressors.
💡 “CLOVERS and CLASSIC both show that restrictive fluid strategies do not improve survival in septic shock. CLOVERS tested early vasopressors in ED patients, while CLASSIC tested fluid restriction in ICU patients. The key takeaway? Individualized fluid therapy based on dynamic assessment is more important than strict liberal vs. restrictive strategies.”
Posted in Medical | Tagged: arise, classic, clovers, egdt, process, promise, rivers | Leave a Comment »
Posted by Dr KAMAL DEEP on April 23, 2024
Navigating Antibiotic Choices in the Face of Diverse Carbapenemase-Producing Enterobacteriaceae
The landscape of antibiotic resistance among Gram-negative bacteria, particularly Carbapenemase-Producing Enterobacteriaceae (CPE), presents significant clinical challenges that require nuanced understanding of both the molecular mechanisms of resistance and the regional epidemiology influencing these mechanisms.
Ceftazidime-avibactam is the preferred choice for infections caused by Enterobacteriaceae harboring OXA-48-like enzymes. The efficacy of this combination is attributed to avibactam’s robust inhibition of OXA-48-like carbapenemases, which enhances the bactericidal activity of ceftazidime.
For NDM-producing Enterobacteriaceae, which often produce class B metallo-β-lactamases (MBLs), recommended treatments include ceftazidime-avibactam plus aztreonam or cefiderocol monotherapy. Notably, aztreonam is resistant to hydrolysis by NDM and other MBLs, but its effectiveness is compromised by co-produced β-lactamases like ESBLs, AmpC, KPCs, or OXA-48-like enzymes. Here, avibactam’s inhibition of these additional β-lactamases restores aztreonam’s activity, making this combination especially valuable in regions with a high prevalence of MBLs.
In the treatment of KPC-producing infections, meropenem-vaborbactam, ceftazidime-avibactam, and imipenem-cilastatin-relebactam are preferred, leveraging their potent activity against class A carbapenemases. Among these, meropenem-vaborbactam is slightly favored based on clinical outcomes and the relative emergence of resistance, as evidenced by available data.
Aztreonam, specifically, is stable against hydrolysis by class B MBLs like NDM, which positions it as a crucial agent against MBL producers. However, its utility is limited when these pathogens co-produce other β-lactamases that can degrade aztreonam. Avibactam, a broad-spectrum β-lactamase inhibitor, counters this by inhibiting serine β-lactamases such as ESBLs, AmpC, KPC, and OXA-48-like enzymes. This dual inhibition mechanism not only targets robust MBLs but also other co-produced β-lactamases, thus broadening the therapeutic efficacy of aztreonam against resistant strains.
It’s important to consider the global distribution of carbapenemases: β-lactam–β-lactamase inhibitor (βL-βLI) combinations like ceftazidime-avibactam and meropenem-vaborbactam are effective against class A carbapenemases such as KPC but are generally ineffective against class B MBLs, including NDMs. The Asian continent, with an estimated 60% of global NDM producers, exemplifies a region where these βL-βLI combinations would be less useful, highlighting the need for alternative therapies in such settings.
The investigational aztreonam-avibactam combination promises efficacy in treating infections that involve both MBLs and other β-lactamases. The dual inhibition mechanism not only targets the robust MBLs but also counters the resistance posed by co-produced β-lactamases, offering a potential therapeutic advantage in regions heavily impacted by these resistance factors.
Understanding the epidemiology of specific carbapenemase genes is critical. Dual carbapenemase carriage, typically NDM co-occurring with KPC or OXA-48-like carbapenemases, is not uncommon and requires astute clinical insight into local resistance patterns for effective treatment planning.
This deep dive into the molecular and epidemiological aspects of carbapenemase production underscores the necessity for tailored antibiotic strategies that align with regional resistance profiles. Effective management of CPE infections depends on the continued advancement of diagnostic capabilities, therapeutic interventions, and an acute awareness of the geographic distribution of carbapenemase genes.
Antimicrobial stewardship is crucial for managing the use of novel antibiotics, particularly in the context of complex infections caused by carbapenemase-producing Enterobacteriaceae (CPE). Stewardship efforts aim to ensure judicious use of these potent drugs to avoid treating patients who are merely colonized rather than infected. This distinction is vital, as inappropriate use of broad-spectrum antibiotics can lead to unnecessary treatment, increased healthcare costs, and the acceleration of antibiotic resistance.
Effective stewardship involves tailoring antibiotic therapy based on precise microbial identification and susceptibility testing, optimizing dosing regimens to maximize efficacy while minimizing toxicity, and shortening the duration of therapy to the necessary minimum. By adhering to these principles, healthcare providers can preserve the effectiveness of current treatment options, safeguard patient outcomes, and reduce the overall burden of antibiotic resistance.
Posted in Medical | Tagged: #CPE # NDM #CRE #KPC #antimicobialresistance | Leave a Comment »
Posted by Dr KAMAL DEEP on August 3, 2023
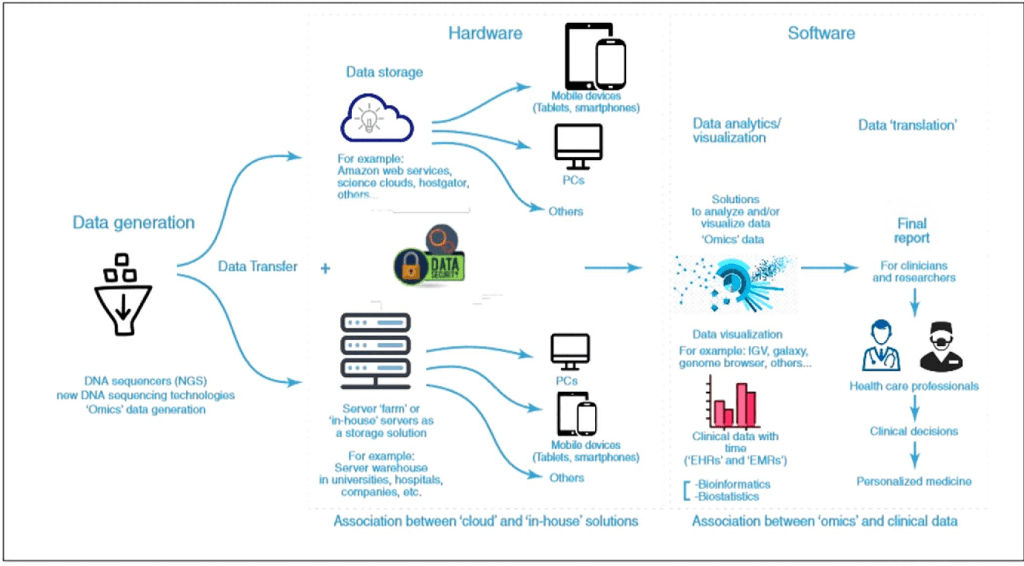
International Congress on Human-Computer Interaction, Optimization and Robotic Applications (HORA) – Importance of Big Data in Precision and Personalized Medicine. , (), 1–6.doi:10.1109/HORA49412.2020.9152842
“One of the very few silver linings about me getting sick is that Reed’s gotten to spend a lot of time studying with some very good doctors… I think the biggest innovations of the twenty-first century will be the intersection of biology and technology. A new era is beginning, just like the digital one when I was his age.” –Steve Jobs (from his biography, Steve Jobs)
Introduction:
As aspiring medical professionals, the journey of becoming a healer is marked by endless learning and unwavering dedication to patient care. In the dynamic landscape of modern medicine, a revolutionary force is reshaping the way we approach healthcare – precision medicine. At the heart of this transformative approach lies the vast reservoir of information known as big data. In this blog, we will explore how big data is empowering medicine students like you, equipping you with the tools to provide personalized, targeted treatments, and revolutionizing patient care.
Conclusion:
As medicine students, you are poised to embark on a transformative journey, shaping the future of healthcare through the lens of precision medicine and big data. The wealth of information at your disposal holds the promise of personalized patient care, diagnostic accuracy, and breakthroughs in understanding complex diseases. Embrace the opportunities presented by big data, and let it be a guiding light in your pursuit of becoming tomorrow’s compassionate and data-savvy healers. Together, we can revolutionize patient care and create a healthier and more resilient world.
Posted in Medical | Leave a Comment »
